

LVNDR Health
LVNDR is a fully remote digital health service providing remote medical services for the LGBTQ+ community, including consultations, testing, medication, and support.
Headquarters
London, UK
Industry
Healthcare, LGBTQ+,
SaaS, Mobile, Web
Duration
8 Months
Role
Product Designer (UX/UI)
Team
2 x Designers
1 x Project manager
3 x Engineers
Responsibilities
—
Product Strategy
—
User Research
—
Visual Design (UI)
—
Interaction Design
—
Prototyping & Testing
—
Design System
📋
TL;DR Summary
Built a foundational product that played a key role in securing $2.2M in funding.
Conducted and analyzed 50+ user interviews and workshops to identify user needs and business opportunities.
Created UX artifacts and deliverables, such as research reports, market research, highly detailed user personas, and journey maps.
Transformed raw ideas and concepts into concrete design deliverables for cross-platform implementation.
Led the development of a design system to ensure consistency and accessibility in design across teams.
The challenge
Our initial research discovered significant issues with the current healthcare system's failure to serve the LGBTQ+ community based on interviews with LGBTQ+ individuals, healthcare professionals, and market analysis.
23% of LGBTQ+ people have witnessed discriminatory remarks made by healthcare staff.
1 in 5 Black, Asian, and minority ethnic LGBTQ+ individuals have refrained from seeking treatment and support.
80% of trans respondents who tried accessing gender identity clinics reported encountering difficulties, with waiting times of up to 5 years.
This audio clip highlights discrimination, judgment, and lack of representation experienced by LGBTQ+ individuals in healthcare.
The solution
LVNDR clinic is a digital platform that aims to improve sexual well-being for LGBTQ+ individuals and modernize sexual healthcare for clinics. The platform offers personalized remote services, including health screening, prescriptions, and consultations by LGBTQ+-affirming clinicians. The platform allows patients to manage their sexual health more efficiently in a safe environment tailored to them. Clinicians can adapt their services to the changing needs of their patients and improve their services using the platform.

The Process
We adopted a lean UX approach to stay within budget and time constraints. We utilized a sprint-based design process to identify challenges faced by LGBTQ+ individuals, healthcare providers, and stakeholders.
Preliminary research
UX audit
Aligning Company goals and objectives
Defining the Brief
User interviews
Affinity Mapping
Thematic Analysis
User Personas
Journey mapping
Minimum Viable product
Roadmap
User flows
Feature mapping
Ideation
UI design
Prototyping
Design System
Collaborating with other teams
Design Handoff
Documentation
Feedback
Usability testing
ℹ️
Note
Discover
Research audit
I started by digging through all the previous work, which consisted of data from multiple quantitative and qualitative research studies and insights from usability testing.
User Interviews
Quantitative Feedback
Over 50% of our interviewees reported experiencing discrimination, judgment, or ignorant treatment from staff during their sexual healthcare.
The average respondent had 3-4 sexual partners per month in a non-covid world.
85% of our interviewees said that dating, sex & sexual health have had a significant impact on their mental health.
No respondents said they used a resource specifically for help with this issue.
Qualitative Feedback
“I am bad with routine, and a drug like PrEP that has to be taken at the same time each day would not suit me because I’ll just continuously forget.” - Ben.
“I’m scared of medical professionals and medical environments. I only signed up to the GP for the first time this year because I needed an appointment, but generally, I’d prefer not to go near them” - Spencer.
“In 2014, I went to get tested for HIV (after a scare), and the doc refused to test me because of my sexuality and his religion” - Liam.
“I wouldn’t feel comfortable going to a GUM clinic and getting a positive HIV result. I couldn’t face the judgment” - Mufseen.
User Surveys
I conducted two different surveys to understand the needs of the LGBTQ+ community and also developed an intuitive medication tracker.
Troglo user survey
Over 44% of people have significant difficulties when managing their emotional and sexual wellbeing
About 65% of people consider privacy and confidentiality when choosing their sexual health service
64% of people feel anxiety and concerns regarding their sexual healthcare
Medication survey
About 45% of people take daily or event-based PrEP
7 in every 10 people struggle with taking their medication on time
Over 34% of people depend on visual queues to remember to take their medication
💡
Key takeaway
Big picture workshop
Next, we conducted a company-wide workshop to build a unanimous understanding of the company values, business opportunities, and long-term & short-term goals. We also did an assumption mapping activity where we created a knowledge base that included the following:
Questions about user behaviors, attitudes, or motivations
Assumptions about these behaviors
Research to test assumptions
Facts based on collected user data
In this workshop, we answered the following questions:
What would make LVNDR a category-leading sexual health business?
Where do these stand on the effort vs impact scale?

Why are we doing this?
What are our short-term and long-term goals?
Who are our stakeholders?
What questions do we have?
What do we need to do to achieve these goals?
What could go wrong?
Why we could fail?
What can we build to achieve these goals?
What is commercially viable?
What would a high-level service map look like?
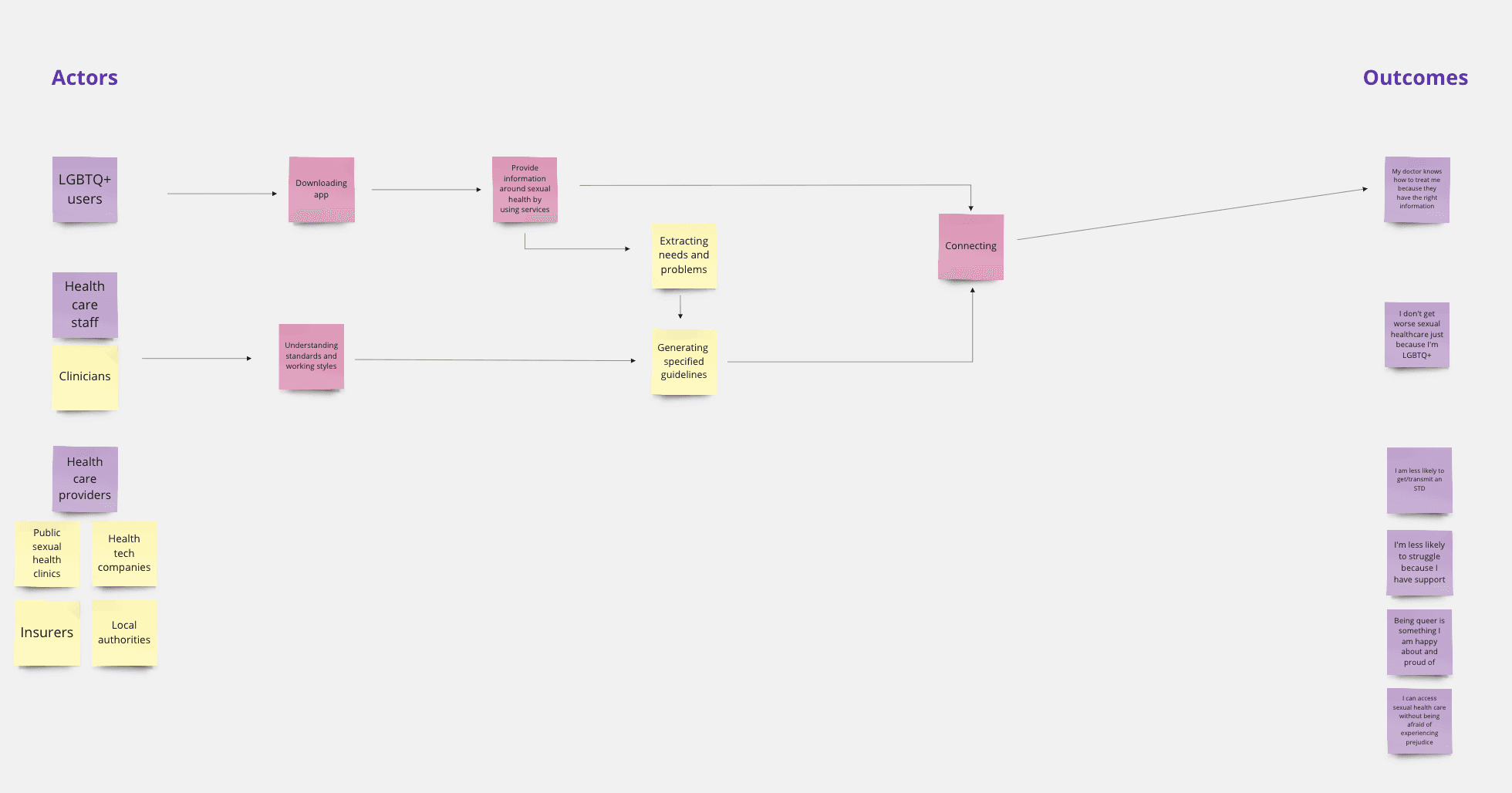
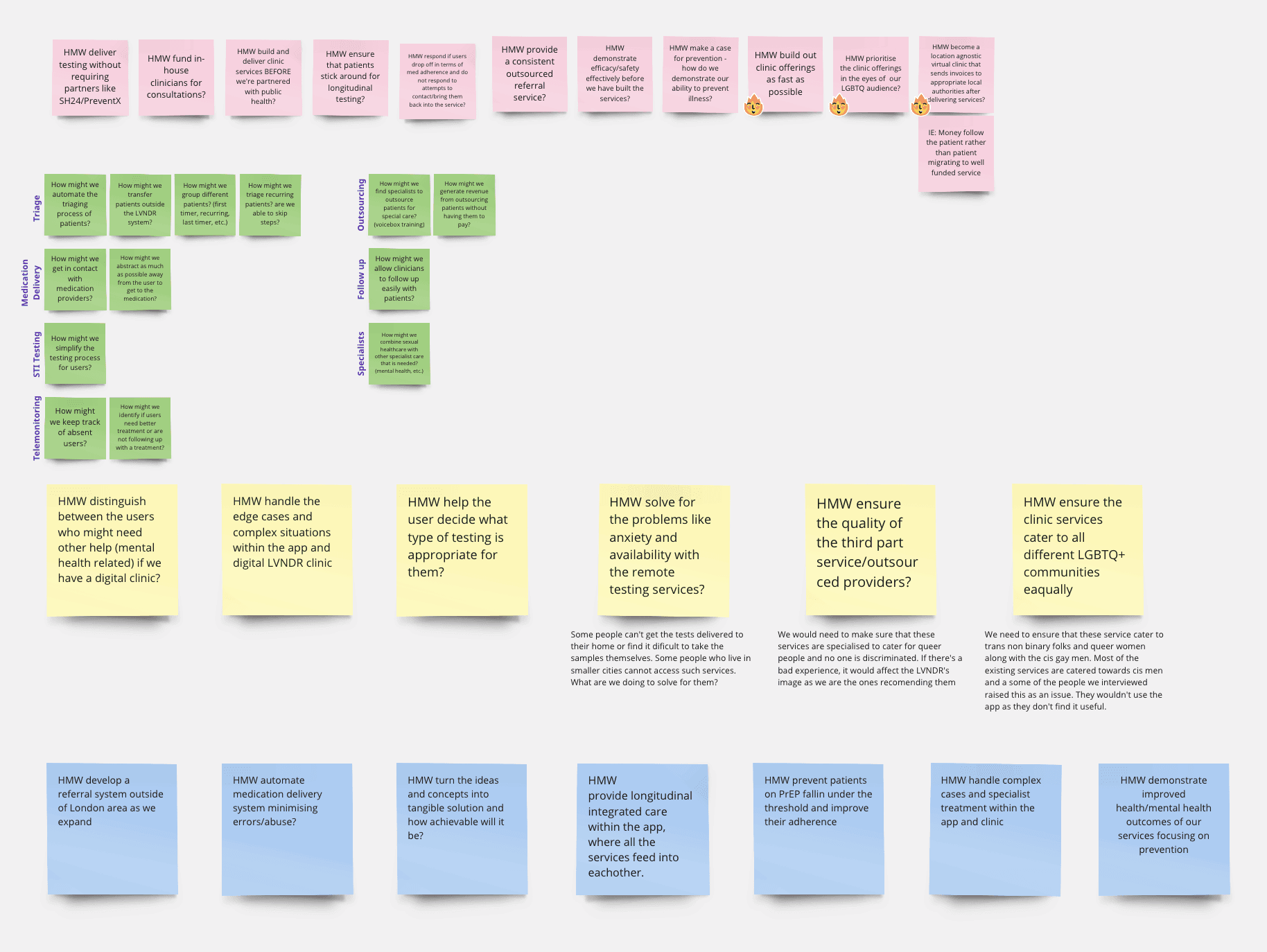
How can we frame the challenges into HMW questions?
User themes
For the healthcare providers, we focused on hiring sexual health clinicians, sexual health nurses, general practitioners (GP), clinic managers, pharmacists, and clinic administrative staff.
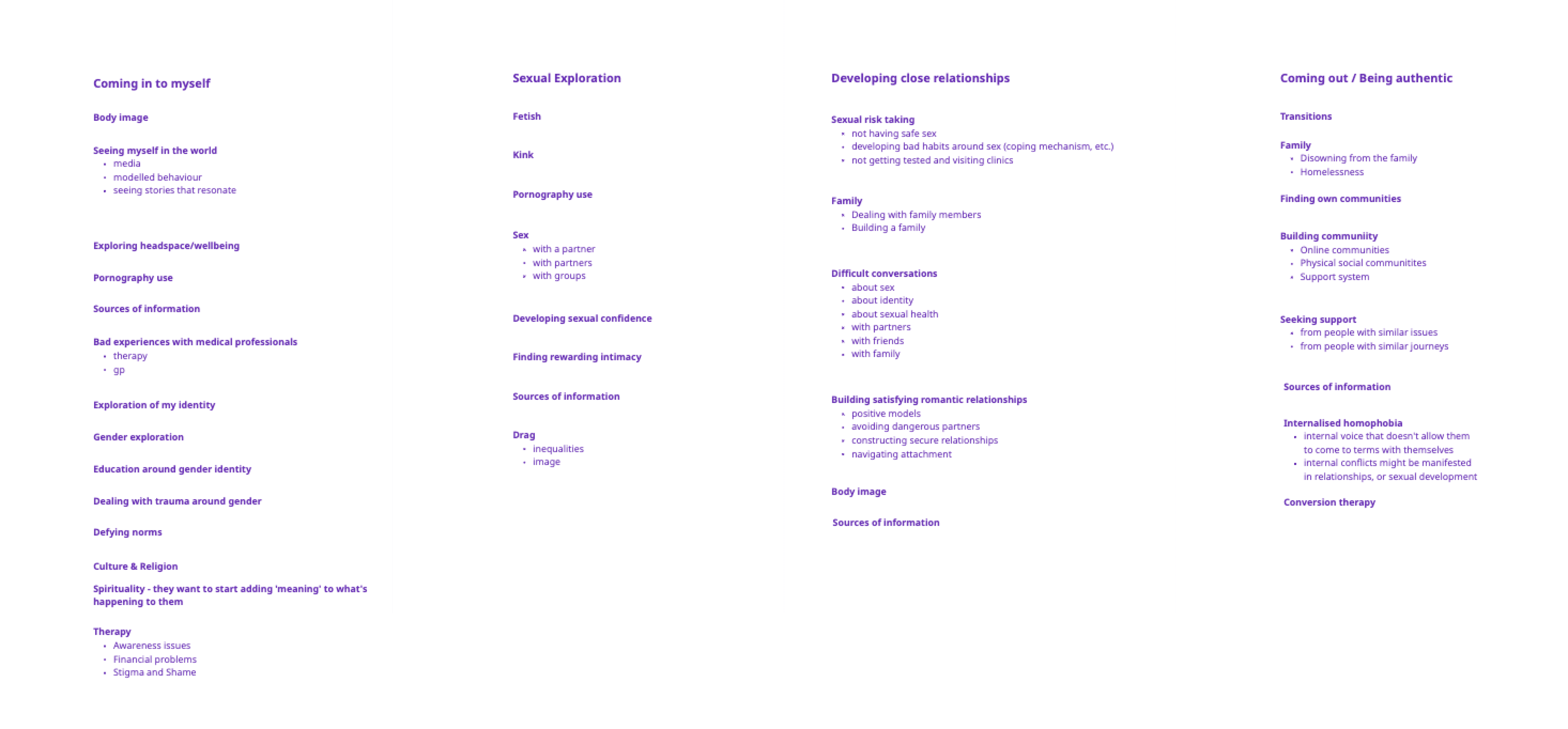
For the LGBTQ+ community, we focused on people with experiences in the following three major themes:
Difficult experiences with identity and self-acceptance
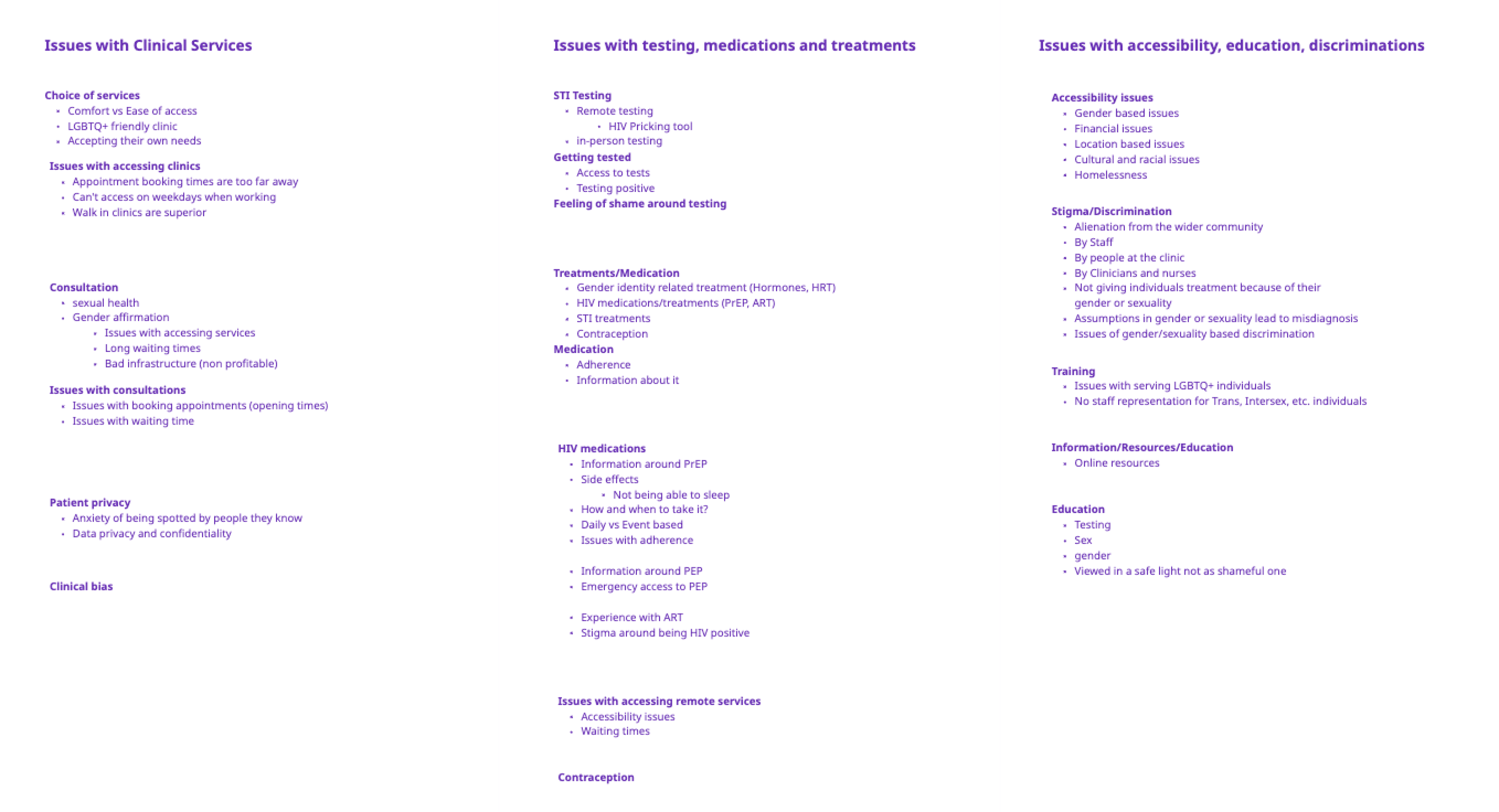
Difficult experiences with accessing sexual healthcare services
Difficult experiences with using sexual healthcare services
Sexual health and mental wellbeing consultations
Sexual health testing - in-person and remote
Experiences around medications (STI medications, HIV medications) and treatments (STI treatments, Hormone replacement therapy)
Getting your medications and treatments
Adherence to medications and treatments
Questions and assumptions
We also conducted a workshop to understand the healthcare provider theme stakeholders. This workshop was conducted for the Product, Clinician, and commercial teams for their subject matter expertise and to align on the questions and assumptions we have. We started by listing the stakeholders in the clinical service provider theme and grouped them into two groups.
Next, we tried to answer the following questions:
What questions do we need to ask about these people to be able to prioritize?
What problems do we assume that we could solve for these groups?
What criteria determine which questions are impactful in progressing us toward our goal of prioritized roadmap?
Finally, we prioritized the questions and assumptions. These were used to plan interviews and hire healthcare providers.
User interviews
We then decided to interview people from the LGBTQ+ community and Healthcare providers to understand their problems better. We agreed on the interview recruitment criteria and produced recruitment plans, discussion guides, and the interviewing process. We worked closely with the Marketing team to recruit people via our previous user groups, social media, and personal networks.
Discussion guides:
The interviews were scheduled and conducted over 4 weeks. We interviewed 30 people from the LGBTQ+ community and 12 interviews with Healthcare providers. All the interviews were conducted online via Zoom, each lasting an hour on average. The interviews were done individually by the members of the Product team. The interviews were assigned to the team members based on their availability and familiarity with the themes.
Some of the topics were very personal and might have been challenging to discuss, so I made sure to approach the interviews with empathy.
Post interview snapshots
We took notes about the interviewee's responses and insights during the interview. The notes were later used as a reference for the Affinity mapping and Thematic Analysis to better understand the context of each interview.
After each interview, we wrote down a summary of insights from the interview. At this stage, we also reflected on how the interviews related to the findings from the previous research, i.e., if they validated or invalidated the existing insights. All interviews were also recorded (Audio) and transcribed using a transcribing tool called Otter.ai. Before the Affinity mapping, we also had to clean the transcriptions, as the tool could not transcribe everything correctly. We also rephrased some of the data to include the conversation's context better.
Define
Understanding the Data
Affinity Mapping & Thematic Analysis
We moved it to the Miro board to make sense of the vast amount of data we collected from the interviews. We conducted Affinity mapping and Thematic Analysis of the data. Affinity mapping included coding/labeling the insights, positive experiences, negative experiences, and opportunities from each interview, looking for patterns and themes, and organizing the data in clusters based on the context of the data. Once we had cleanly labeled data organized in clusters, we conducted a thematic analysis. This included creating new labels that encapsulate potential themes, looking for themes in the data grouping, and evaluating the themes. This process was iterative, and we kept revisiting the data to refine the labels and themes. This process was done while we were interviewing and afterward. It was the most time-consuming part of the process, taking over 4 weeks of an iterative process.
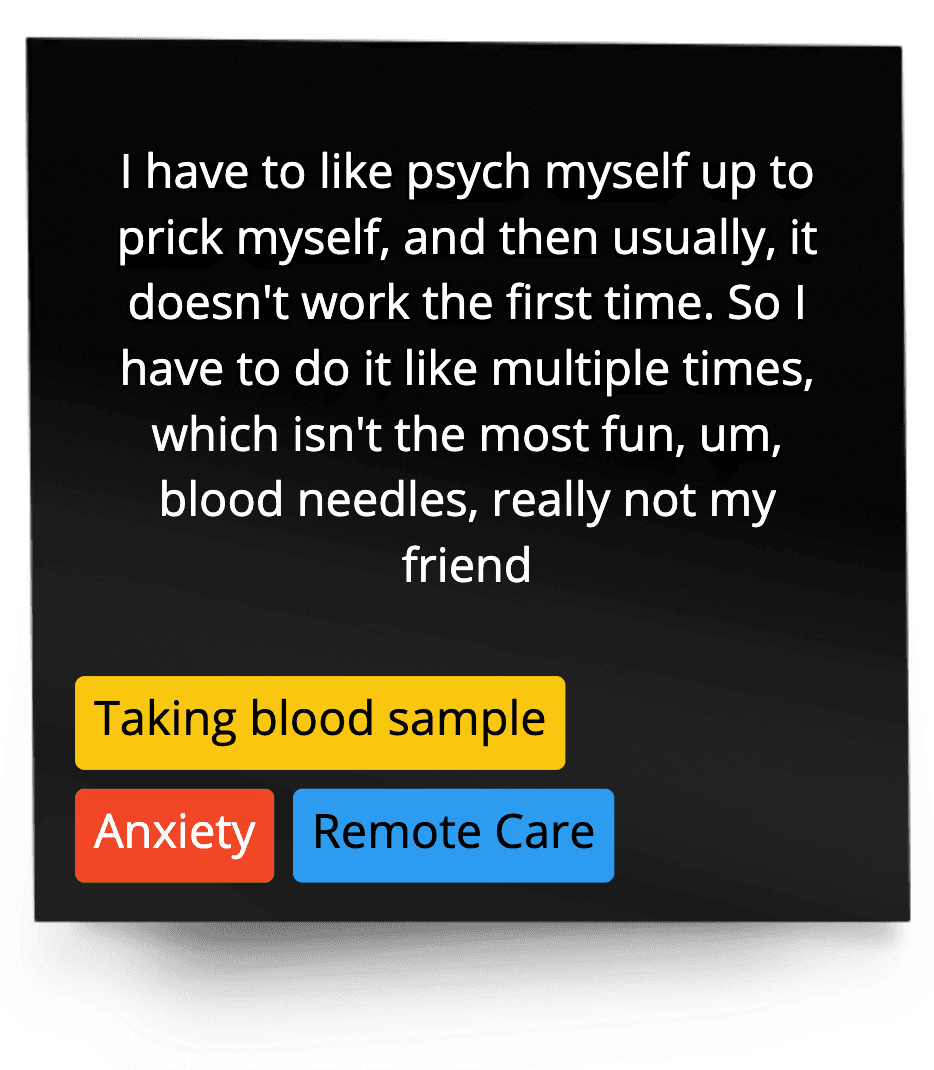
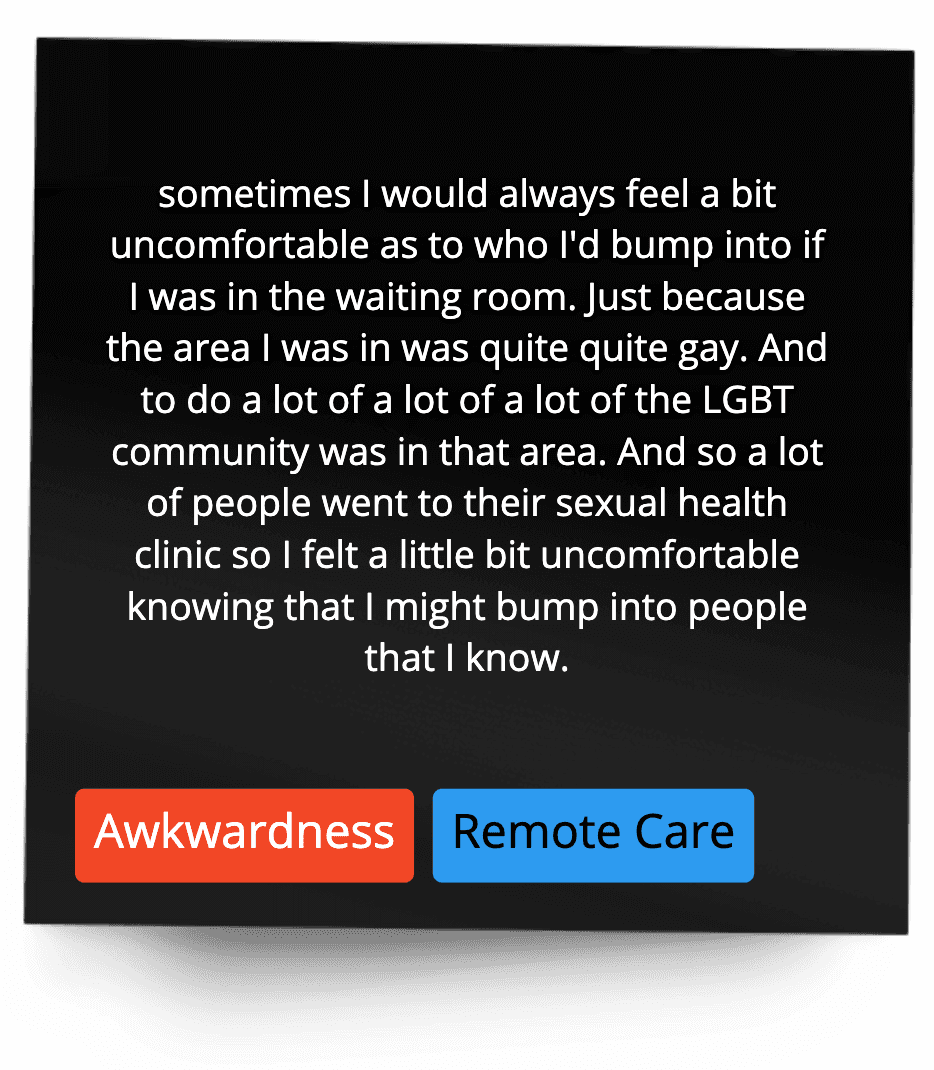
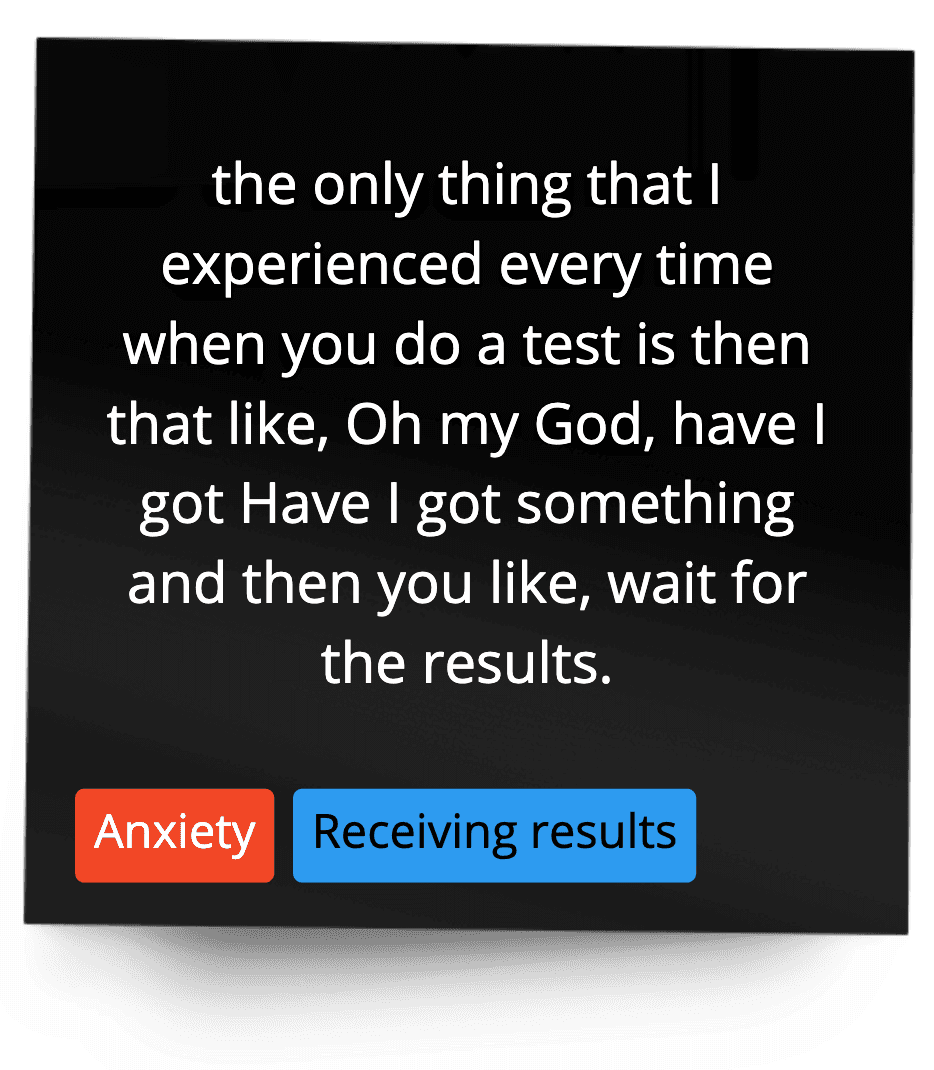
User interviews data examples





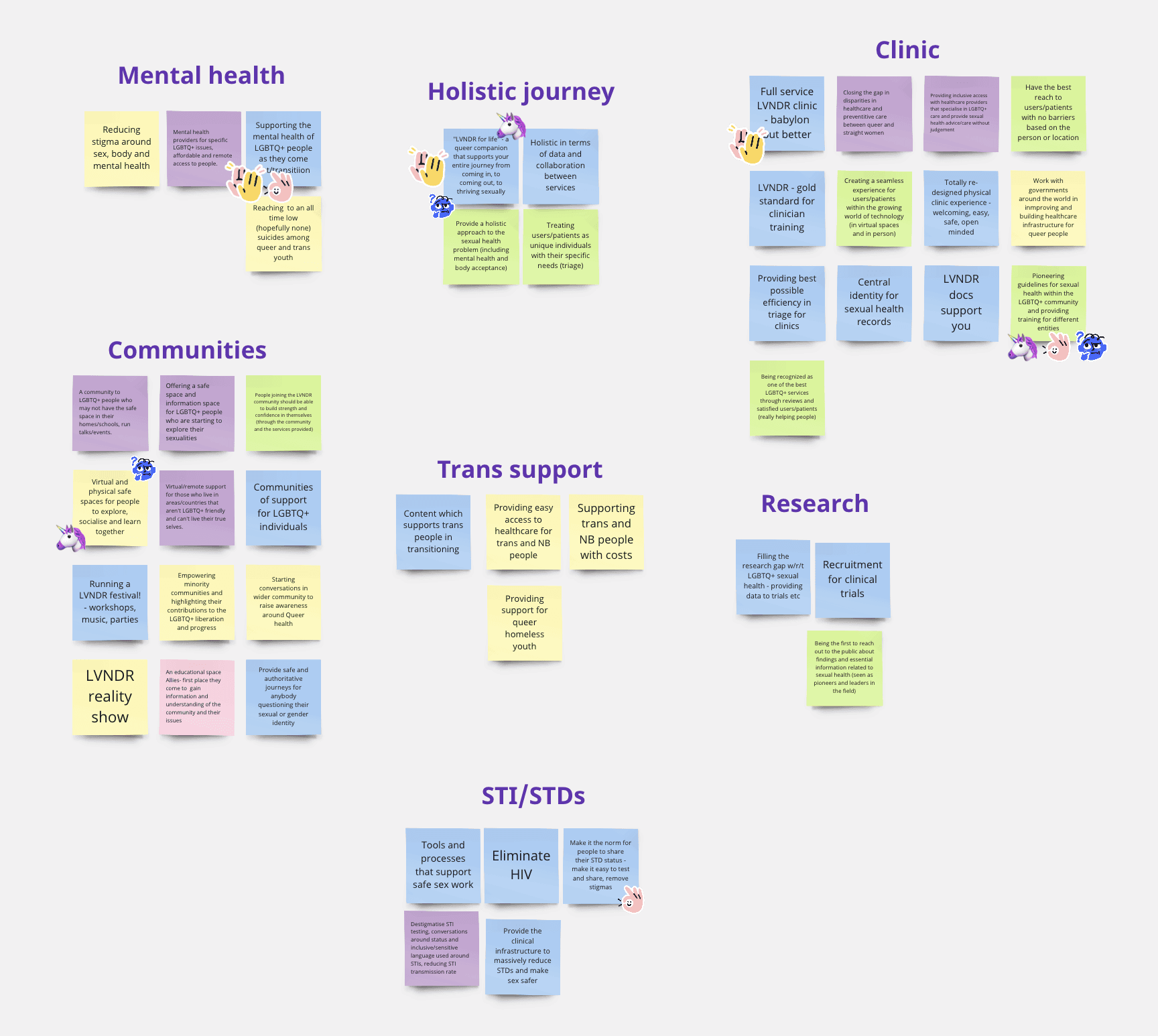
High-level Persona Building
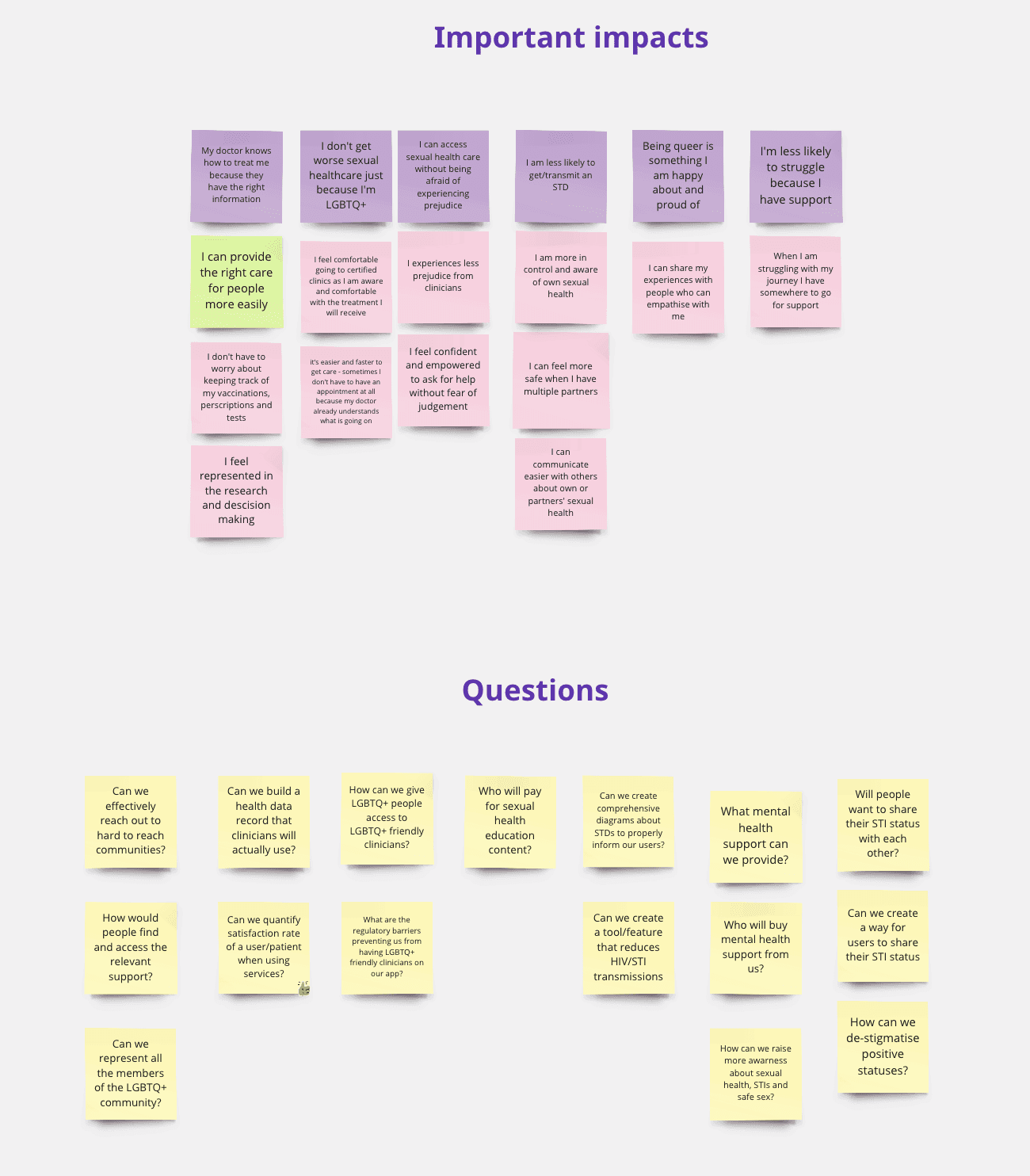
Building persona statements based on the user themes and the interview data from thematic analysis. This activity aimed to list persona statements for all the problems we saw in the interviews. Once we had a board of many persona statements, we looked for overlaps, merged similar ones, and grouped them into themes. Next, we prioritized the persona statements based on the following criteria:
How much does the problem affect the person’s health or mental well-being?
How long does the problem take the time away from the person?
How much change does the person experience when going through the problem?
How much does the problem impact the persona’s understanding of their health or accessing the service?
What problem can LVNDR solve for? How much effort does it take?
Persona statements

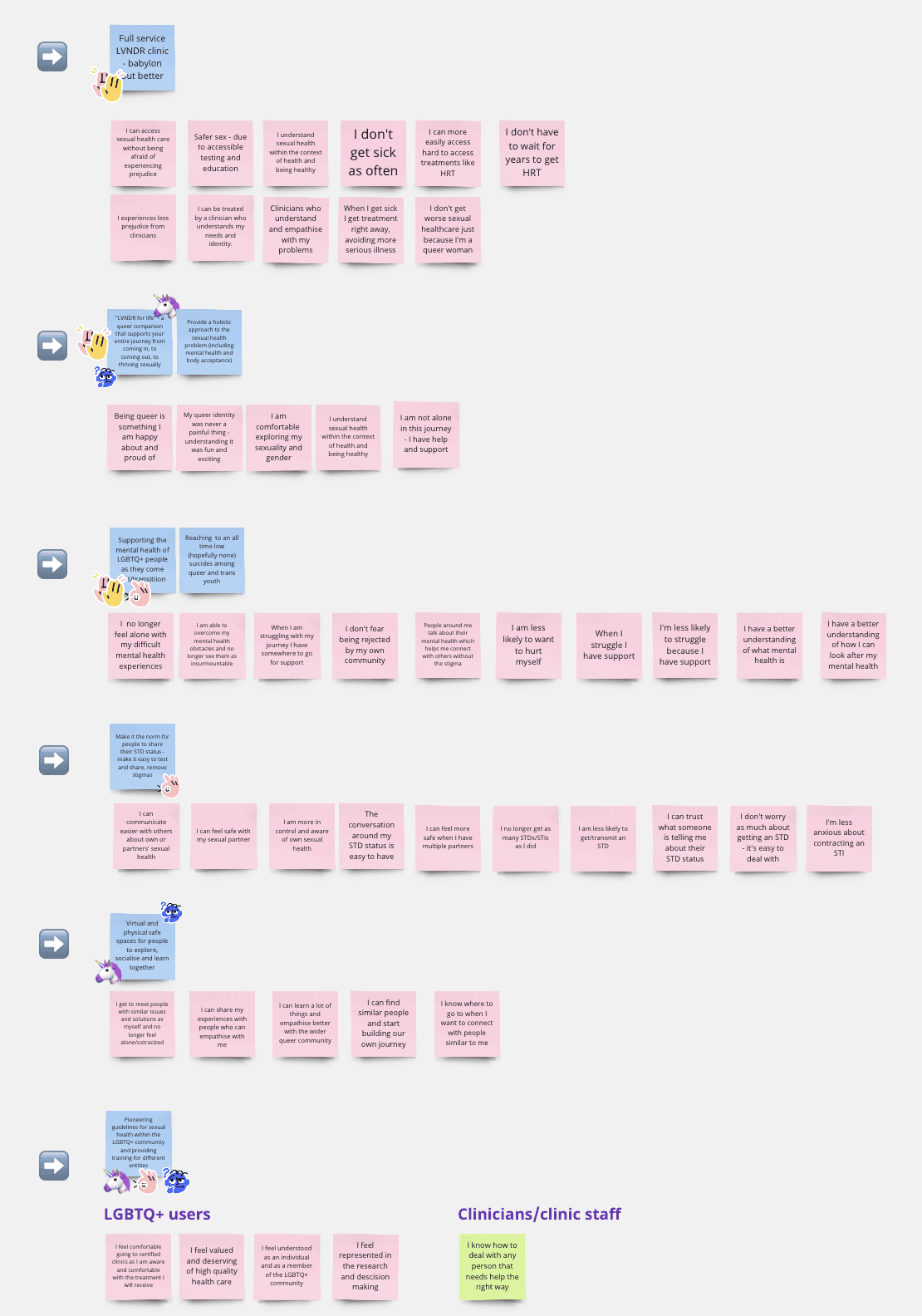
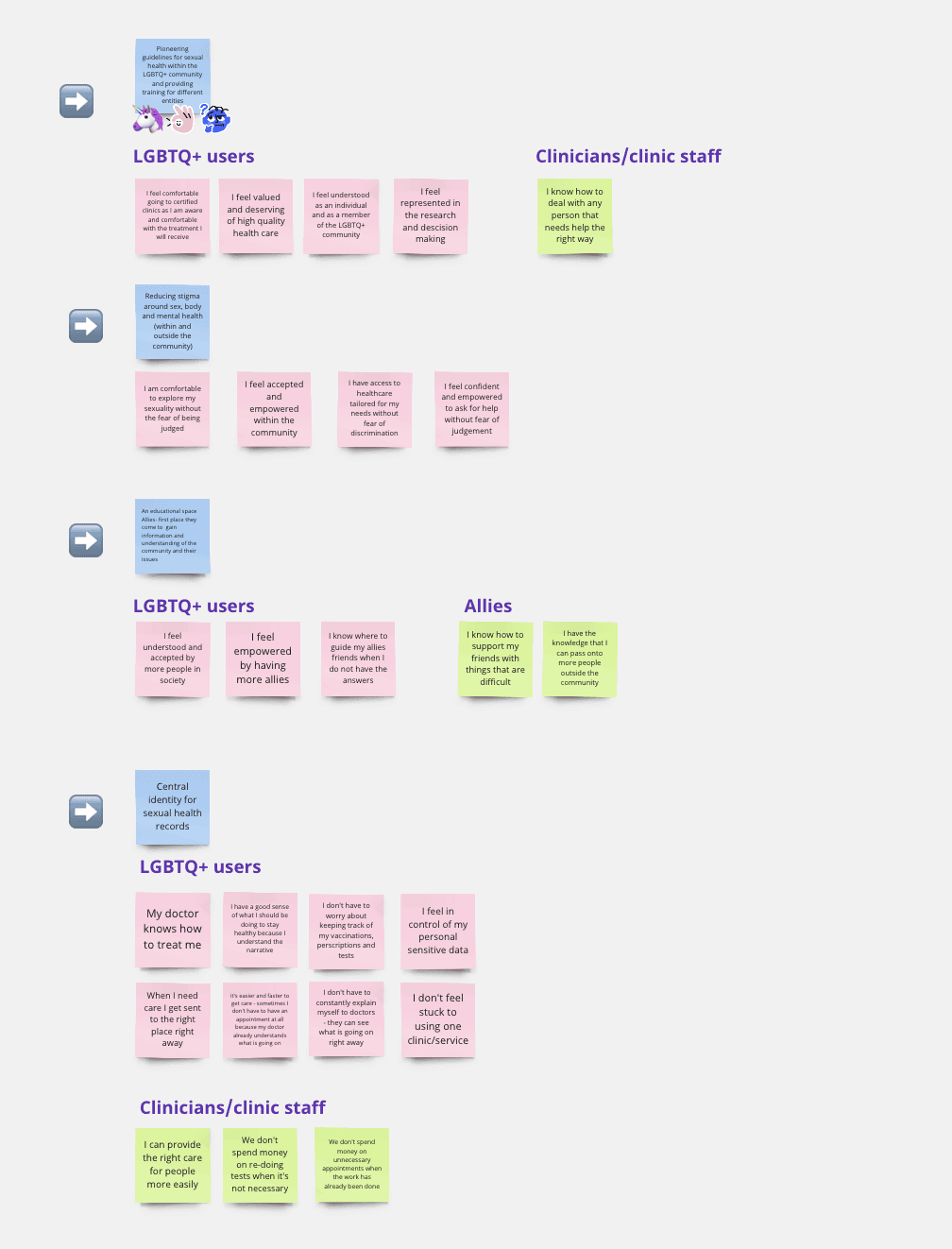
High-level User stories
The product team then used these persona statements to write user stories for each statement. A user story involves each persona statement and their journey of the positive or negative experience. This was to quickly map out the assumed journey for each persona based on our understanding of the old research, interview data, and the problem space. This later helped us prioritize what we could realistically work on and what we wanted to focus on first.
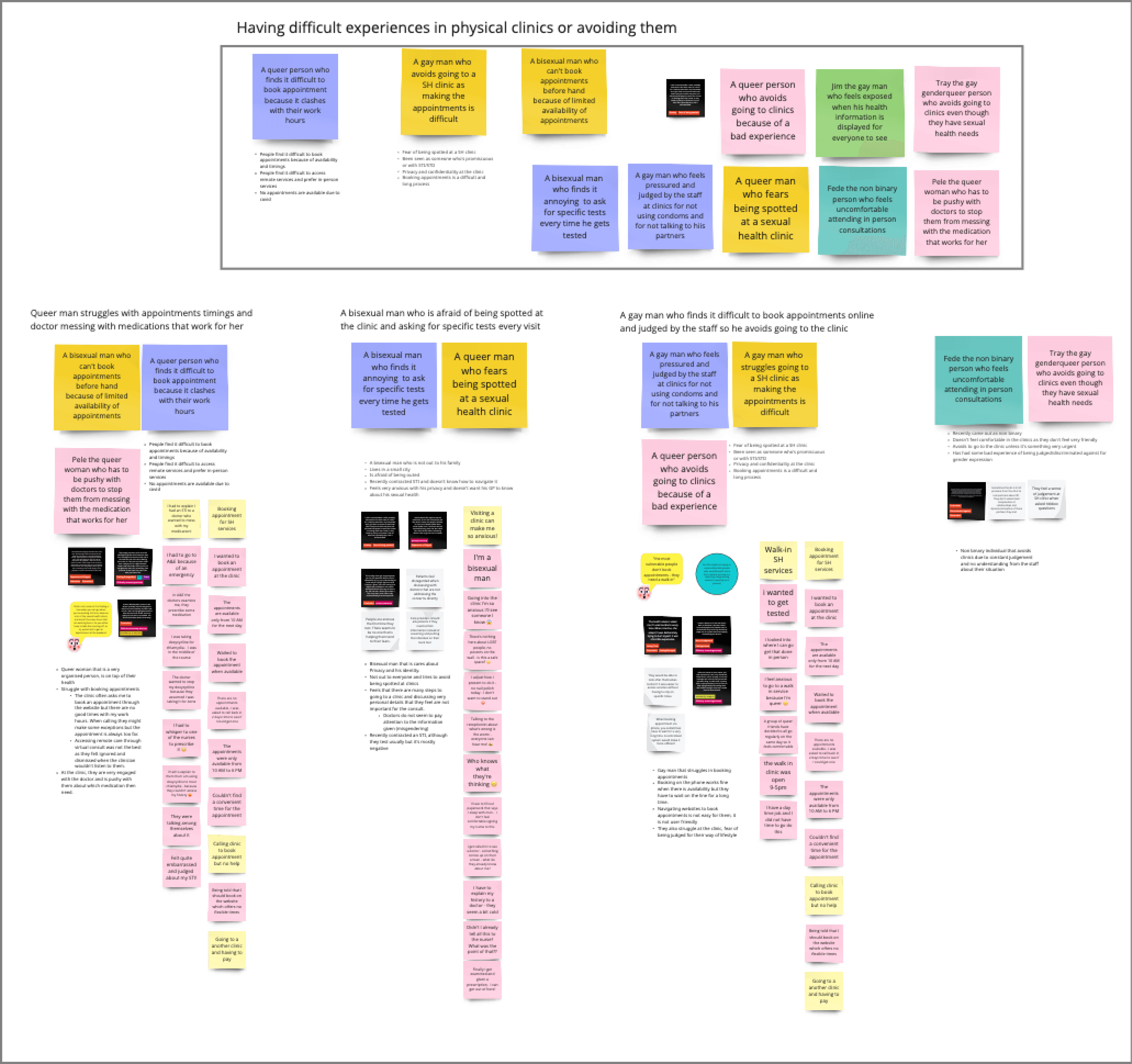
Problem consolidation workshop
A team workshop will be held to bring together the persona statements with the highest priority, the interview data, and team assumptions. It was to consolidate the original problem stories into problem statements that we can easily understand and use for prioritization. It was also a more accurate representation of the experiences of the people we interviewed and was used to build our personas. It was done by teams divided into smaller groups that were given persona statements, which they had to map to the interview data. It was the first time all the teams saw the interview data, and it helped them understand the problem from the user’s perspective and build empathy. We used the 1st half of the workshop to help us understand and familiarize ourselves with the interview data, and the 2nd half was used to map the persona statements to the data and build problem themes.
This activity was different from high-level user stories activity because:
The user stories were based on the product team's understanding of the data and problem space, which made them vulnerable to the team's biases and assumptions.
The user stories were quickly put together, narrative-driven, and did not accurately represent the users.
They also lacked the consideration and input of experts from the clinical and commercial teams.
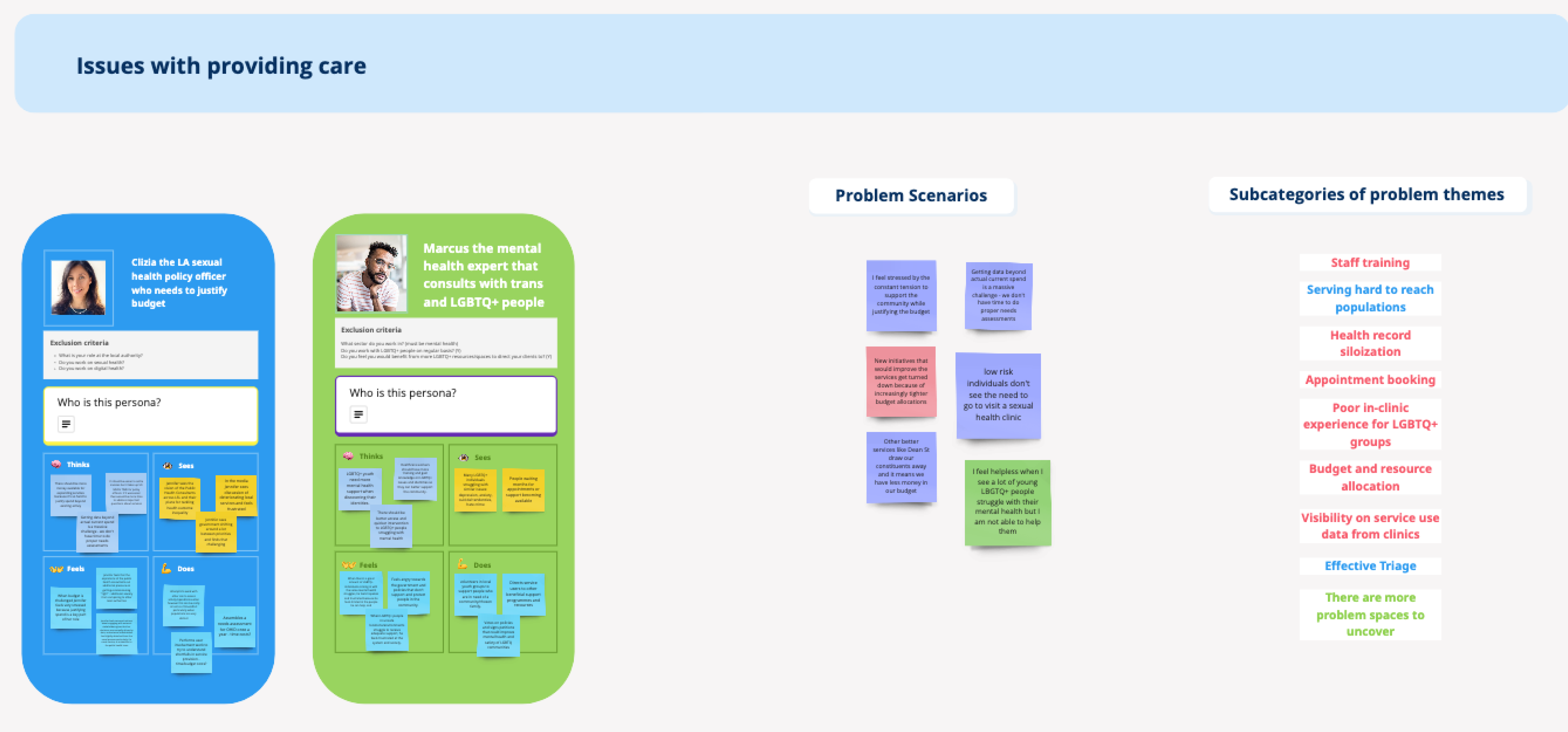
Problem Themes
As a result, we discovered three major groups of potential users and the problem themes for each group.
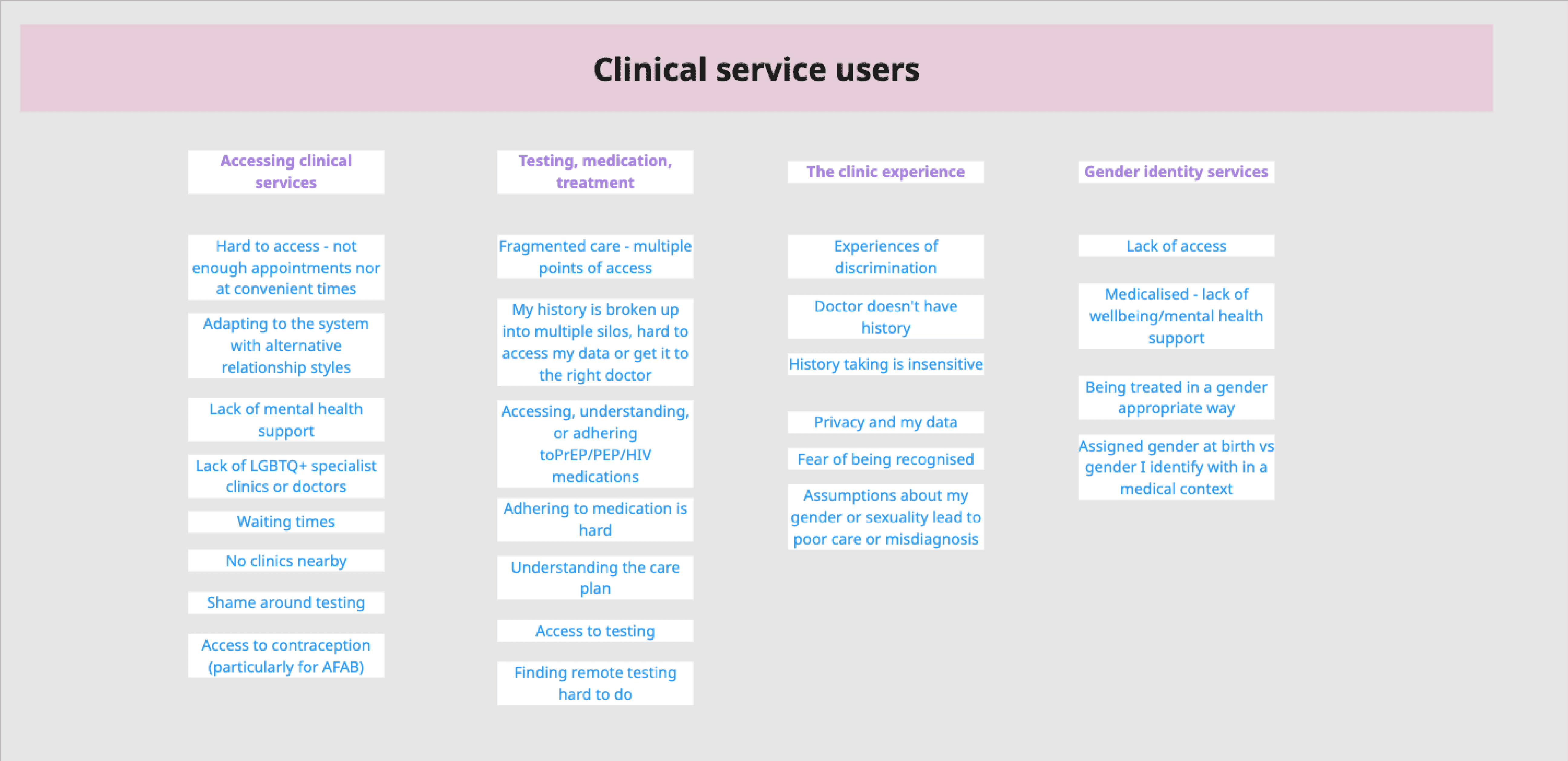
Healthcare providers: Sexual health clinics, Clinicians, GPs, LAs, and other healthcare staff.
LGBTQ+ people are concerned with clinical services.
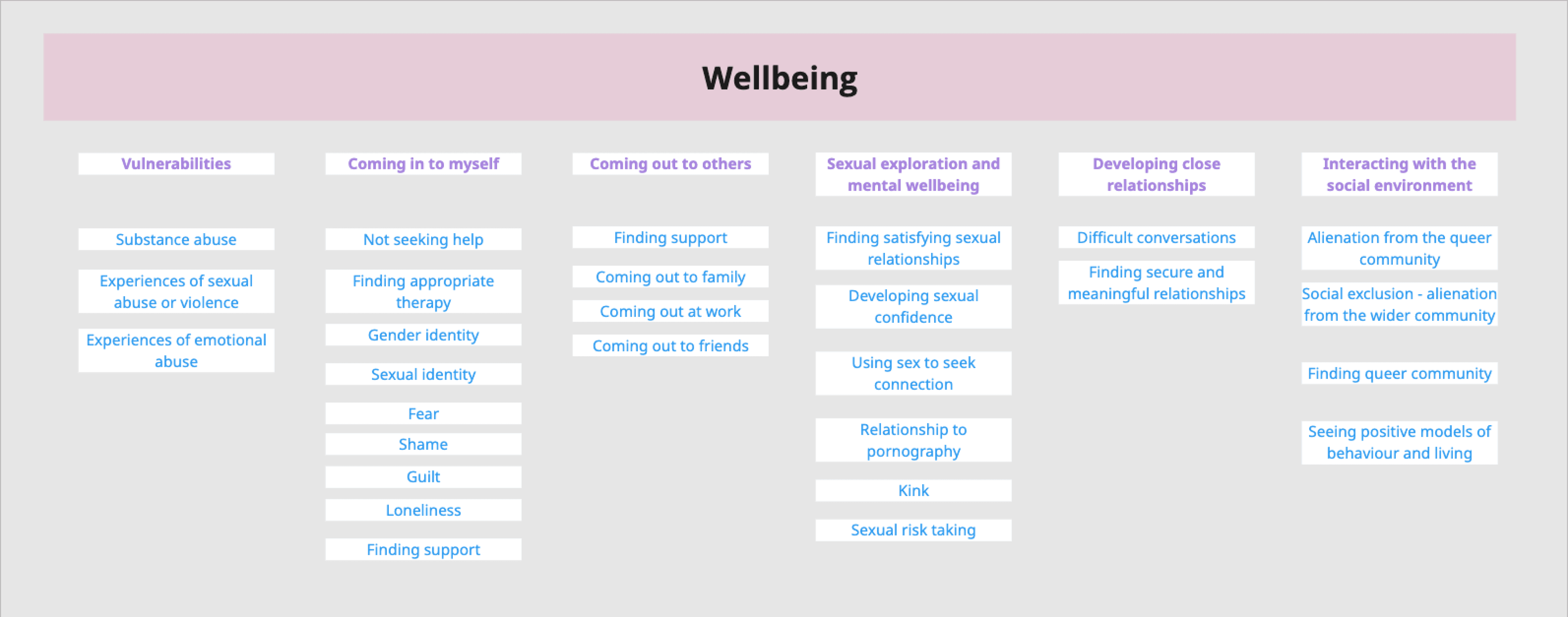
LGBTQ+ people concerned with Identity and Wellbeing.

The product team then refined and restructured these themes, considering the research insights and input from the other teams.
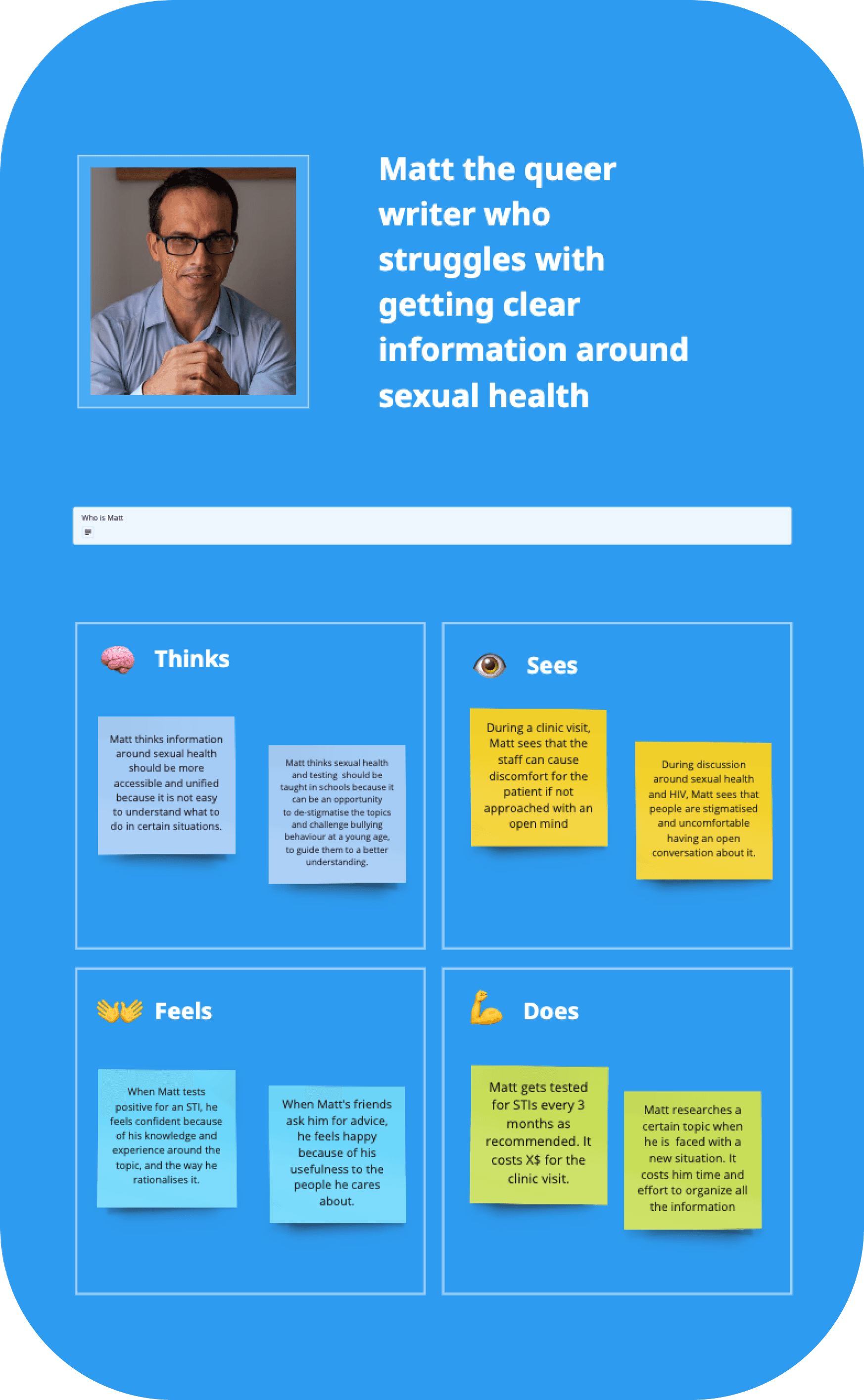
Understanding the Users
Museum of Problems workshop
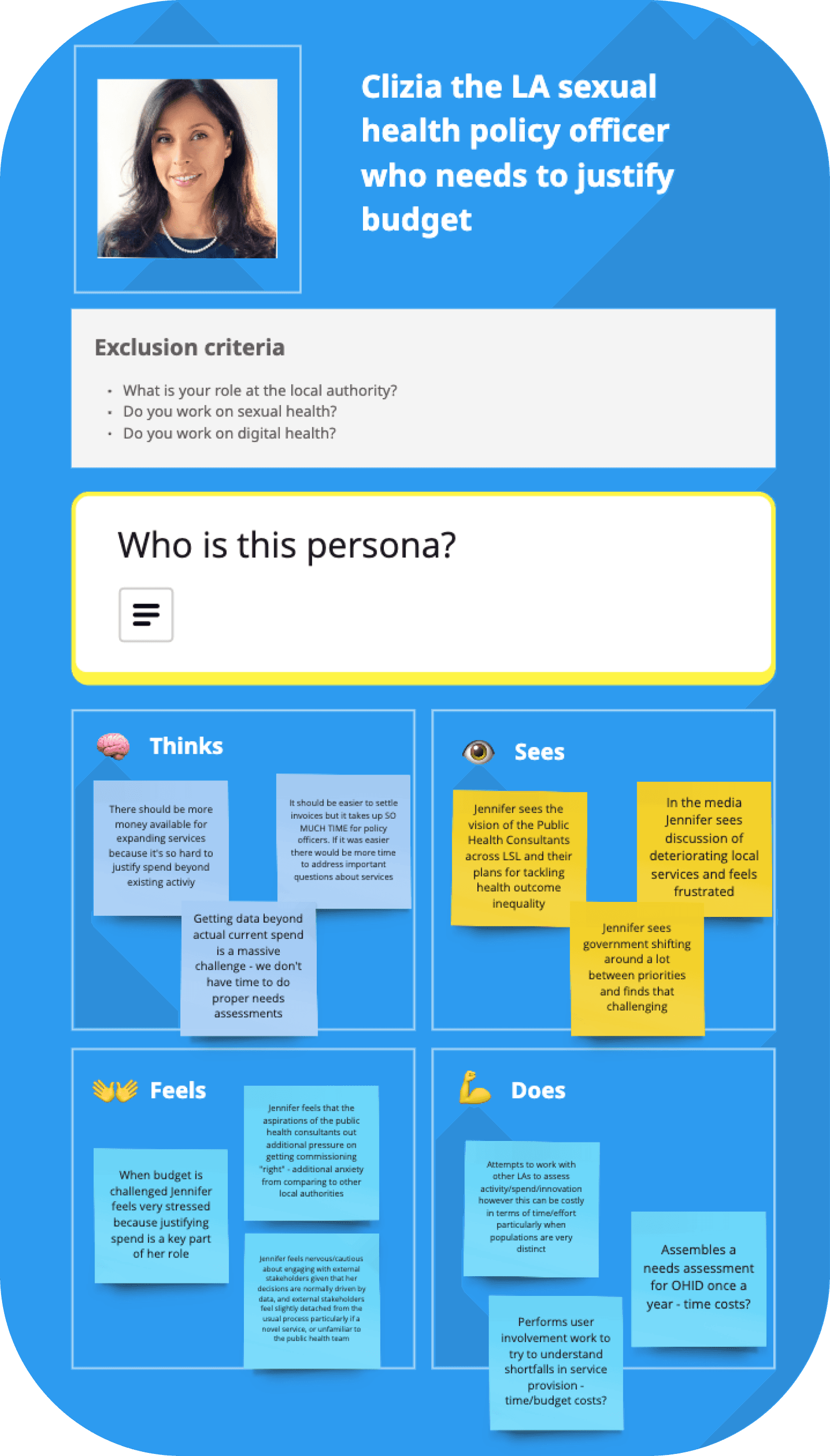
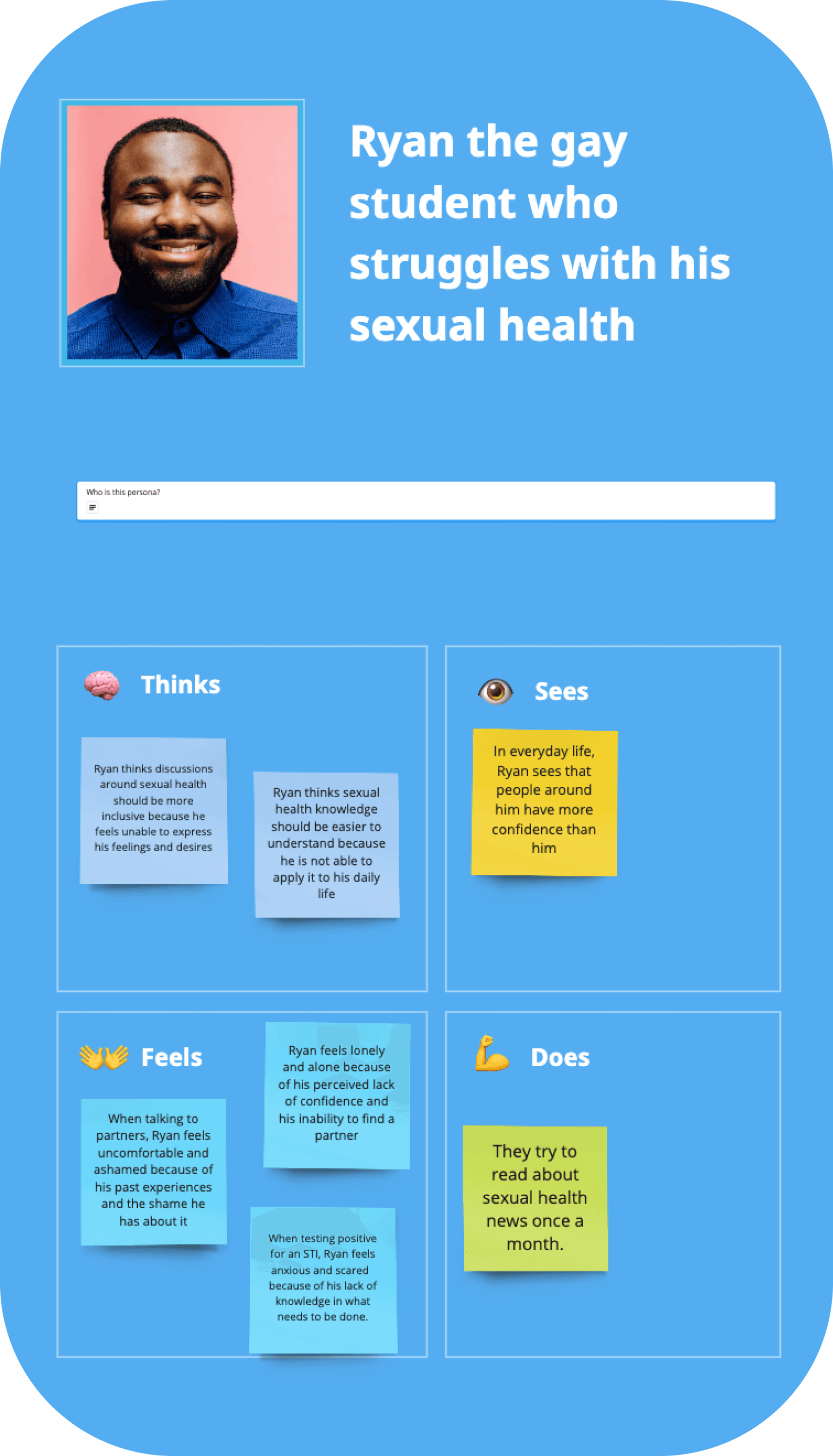
Next, we conducted a cross-team workshop to build the user personas. We divided the highest priority persona statements into six different problem theme clusters. The teams were divided into three groups, each working on two problem theme clusters.
Each persona had three sections.
Persona identification: This included the persona statement with a name, a picture, and the exclusion criteria to determine who they are based on a set of questions.
Persona description: This is a detailed description of who the persona is, what kind of person they are, their story, their interests, and their problems. This section is very descriptive and makes the persona vivid and real.
Empathy map: This is split into four quadrants (Says, Thinks, Does, and Feels), which provide a glance into a user's overall personality.

The group also tagged each of the personas based on how the persona related to their knowledge of the data and their ability to pull the corresponding data from the research.
Hypothesis: These personas were based on the subject matter expertise of team members (clinical team, product team), but they did not have or were unable to find corresponding data.
Somewhat confident (needs more data): These personas required more data to support their accuracy but already had some supporting data.
Seen in the data: These personas were based entirely on the data.
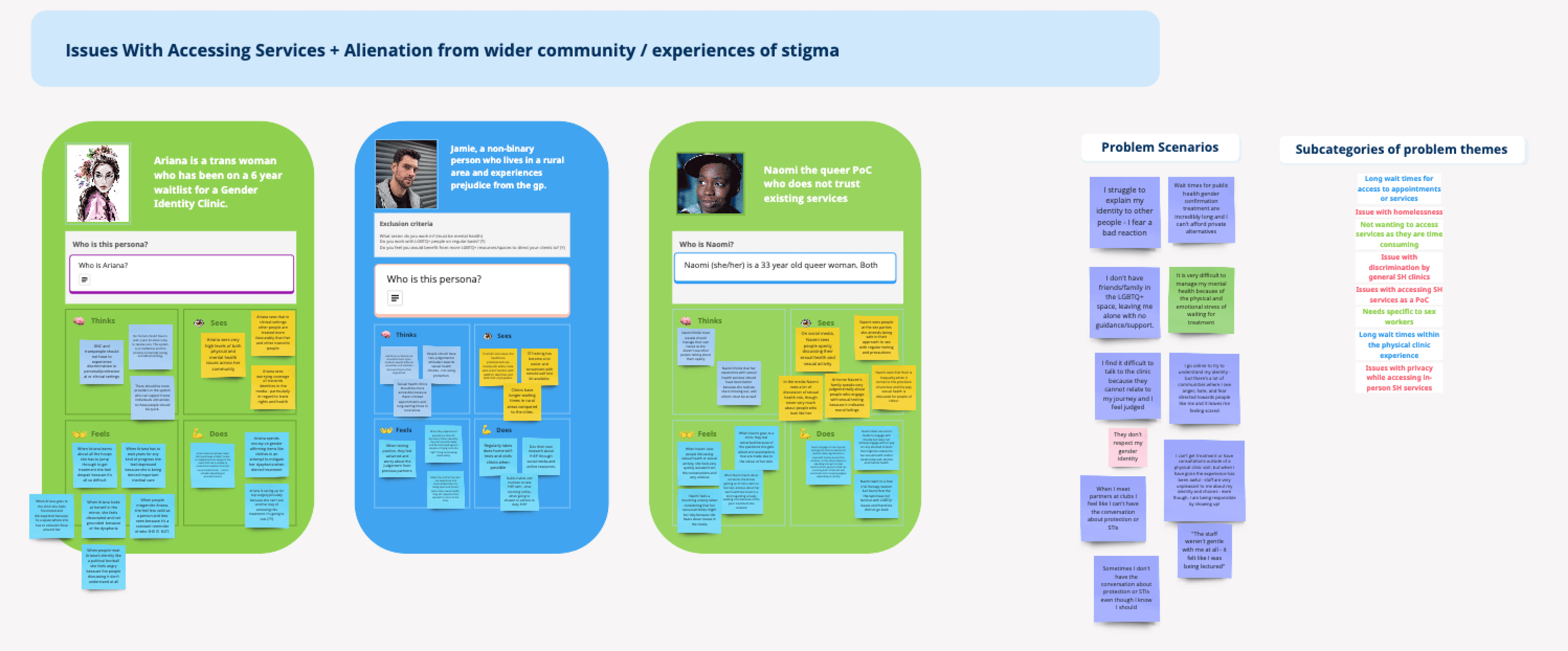
Each group added corresponding problem statements and problem themes to the personas. They also answered the following questions for each problem theme
What’s exciting/interesting/surprising about this problem space?
What evidence or knowledge can you bring to build on this?
What questions or gaps in our knowledge do we still have?



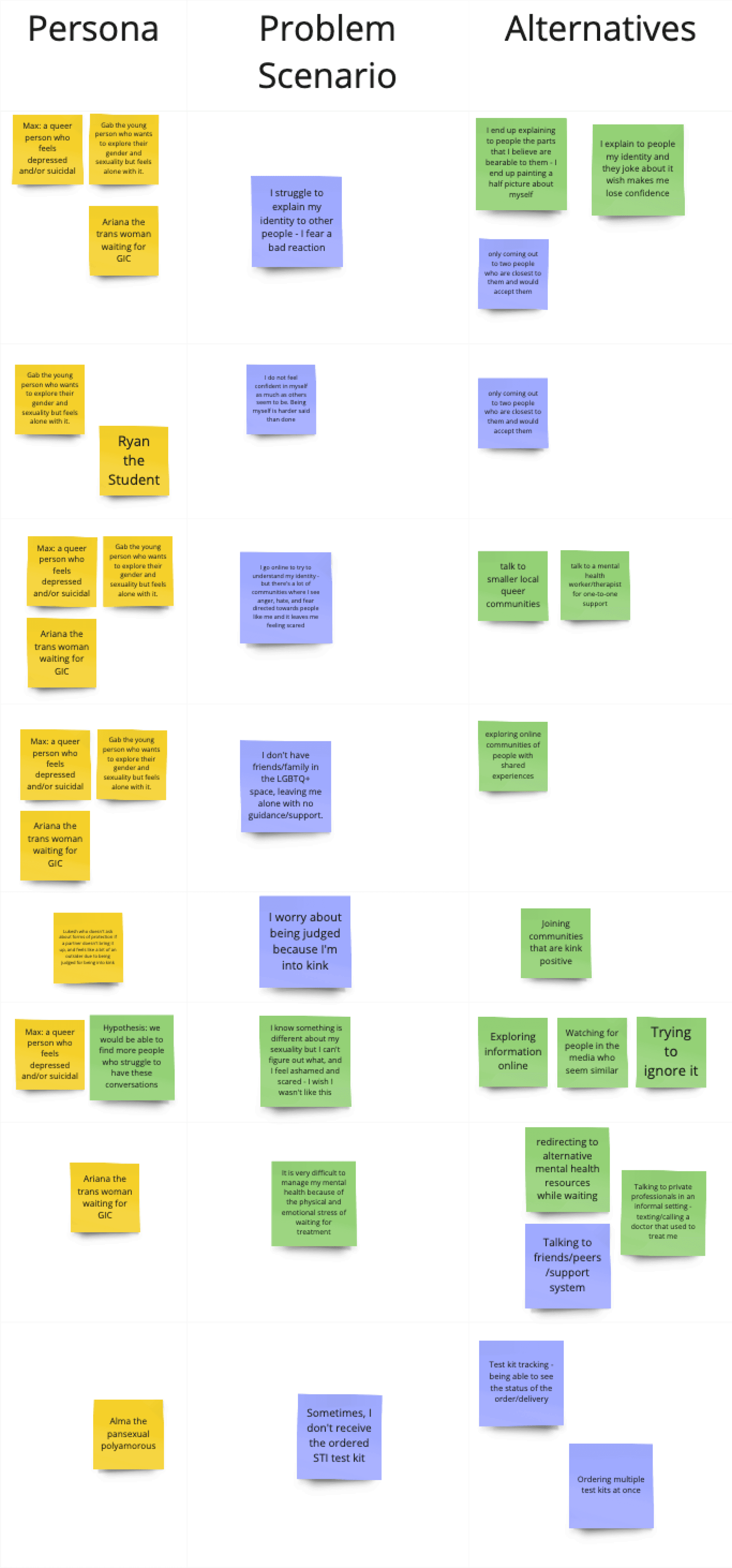
Problem scenarios and Alternatives
Next, the product team worked on the remaining personas from each problem theme. We then started grouping problem themes and corresponding personas. We took the grouped personas and added problems, themes, and alternatives. This allowed us to see all the problem themes and their relation to different personas and also understand the current options available to them. This gives us deeper insight into the persona’s problems and their journey.,

Museum of Problem Stories workshop
The next workshop was to build detailed user journeys for different personas. This was divided into two workshops: one focused on well-being personas and the other on clinic users and providers. For each workshop, we created four groups based on the team members' roles. Each group consisted of members from each team: clinical, Commercial, Product, Marketing, and Engineering.
The first activity was to align the criteria to consider while creating the journey mapping. Next, each group was given a set of persona statements and related outputs such as user personas, problem statements, user stories, problem themes, interview data, and Journey mapping templates. Each group mapped out the journey in detail for different problem statements for each persona assigned to them with the corresponding quotes from interviews and assumed thoughts and feelings of the persona in their journeys. At last, groups presented the outputs to everyone and came together to prioritize the problem.
This resulted in detailed User journeys that built a deeper understanding of each user persona and their journeys. It gave each persona context as to what their problems are, what solutions they are currently using, what opportunities we have, and what challenges they face in solving these problems.




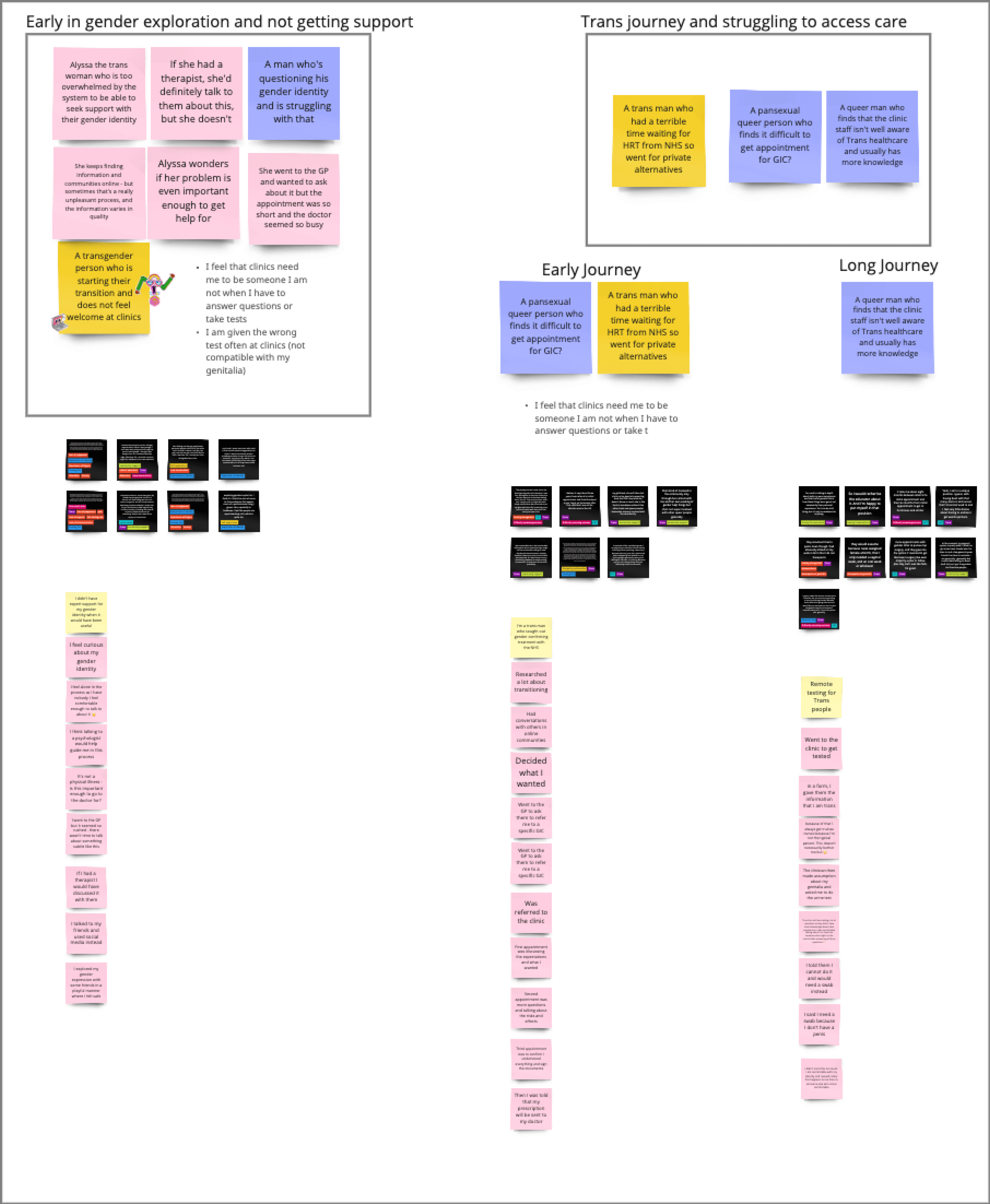
Personas and Journey Maps
The product team later conducted a similar workshop among ourselves to finish the remaining User Personas and Journey Mapping, resulting in the creation of 30 detailed user personas and various corresponding journey maps. When working on the solutions, all different teams used these design outputs to go back to the what, who, and why of the problem space. This was extremely helpful for the product team and the clinical, commercial, marketing, and development teams.
Expert sessions
We also conducted various expert sessions where we presented the user personas and journey maps to the professionals who work with similar people. We also received insights and feedback to fill the gaps and validate the data. For example, we presented well-being theme personas to various psychotherapists and psychiatrists who gave us invaluable feedback on how they relate to their patients, validating the journey maps and problems they face in providing care for them. All this feedback and insights were used to improve the user personas and journey maps and were also used later on during the ideation and designing phase.
ℹ️
Note
Sinuo (UX/UI Designer) left our team during this phase. At a later stage in the Design phase, Soraya (Product Designer) joined the team. In between these, I was the only designer working in the team and leading the design process.
Product offering
Features ideation workshops
Value Proposition workshop
We conducted a workshop with the teams at LVNDR to align on our value proposition and ideate on what LVNDR's product offering could be. Team members were divided into three groups and were instructed to write down our value proposition statements and all possible solutions that could solve the problems of our users based on the following questions:
How Might We enable and encourage LGBTQ+ people to access meaningful support when facing shame, guilt, and isolation in the journey of coming into themselves?
How might we make accessing clinical services like consultation and testing quicker and easier without experiencing stigma?
How Might We improve the experience of remote care, follow-up, and comprehension of care plans through better-designed digital tools that are less labor-intensive and time-consuming for clinicians?
How Might We improve the process of taking and using patient histories and the relationship service users have with their health data in sexual health services?
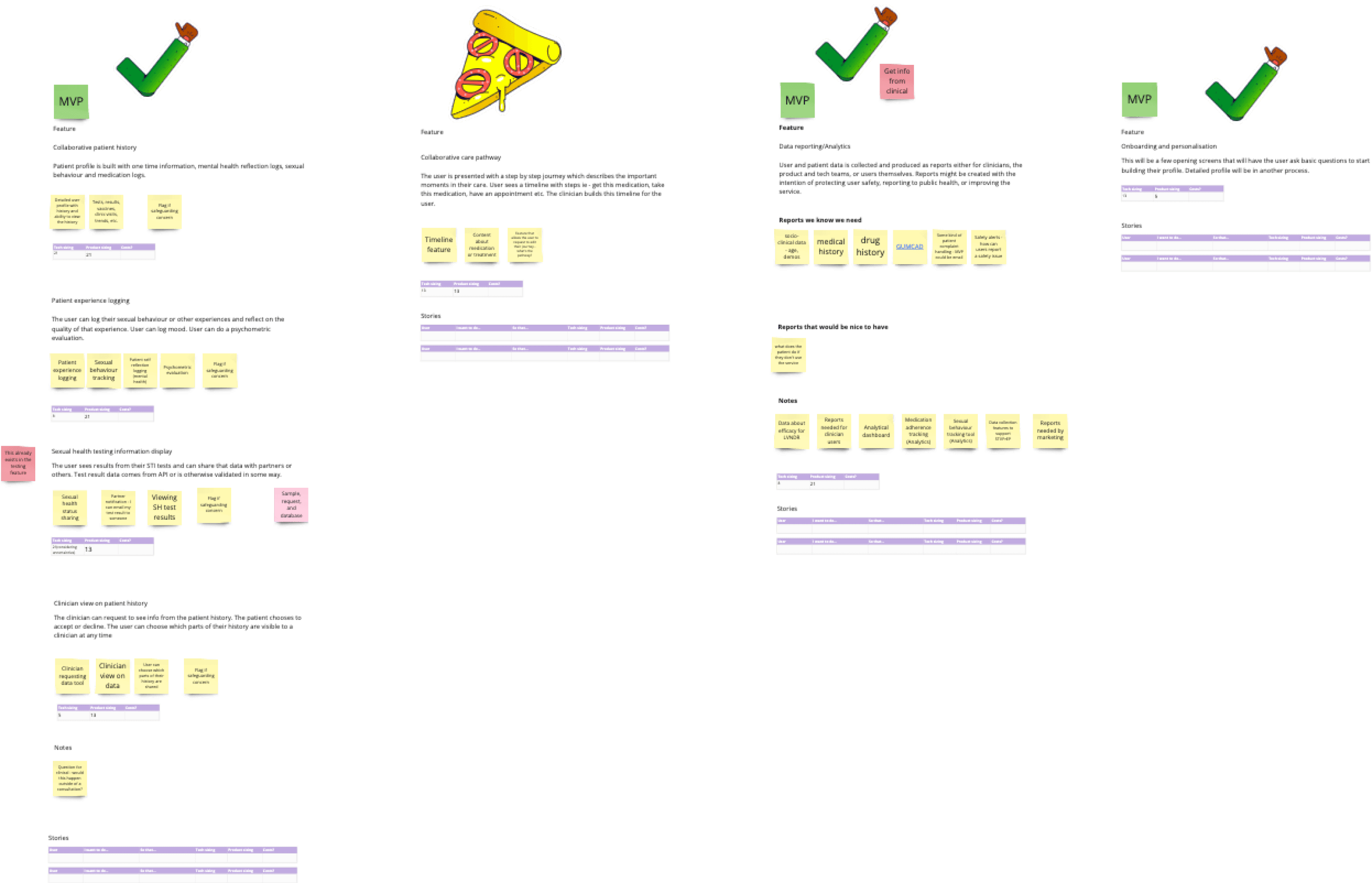
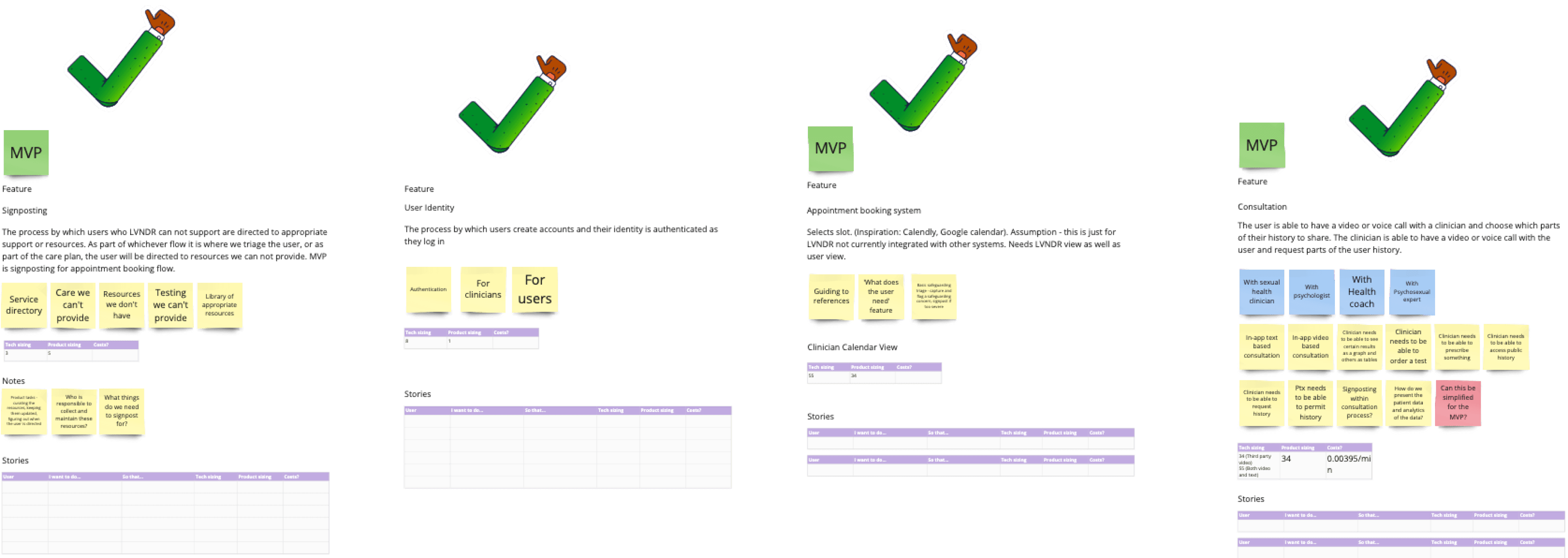
The outputs were three versions of high-level service maps of LVNDR's product offering. After presenting and discussing each, we created a feature list describing the features we could build, the challenges and limitations, and the Product and engineering team's sizing (how much effort, time, and resources were needed to make it). The sizing was done using agile story points.

Next, we conducted a Metrics mapping workshop, during which we decided on the North Star metrics. We also aligned on the business outcomes, Clinical outcomes, and User problems to discover the overlap between the three, which would be our highest priority goal. This helped us better define and prioritize the features among all teams.
The features were prioritized based on their impact on the user (the value they bring) and the effort required to build them for the business.
Defining features & sizing

Considerations: constraints and opportunities
CQC registration
Any organization that provides regulated activity (healthcare and social services) in England must be registered with CQC. The commercial and clinical teams were working on securing this registration/approval. This registration process takes some time, so we had to prioritize the features for phase 1 that do not require CQC registration first. Other features were moved to phase 2 to ensure we adhere to the regulations.
Signposting vs. in-house services
Features like STI testing, prescribing medications, and delivering medications require a lot of resources to build. These features need an end-to-end implementation, including hiring qualified healthcare professionals, pharmacy and delivery centers, and processes. The alternative is to signpost the user to another service provider or partner with the providers for integration. All of the alternatives come with their challenges and limitations.
Public healthcare system
Working with public healthcare systems such as the NHS benefits the users, resulting in free or cheap services. However, this comes with its challenges. The NHS is not designed well to provide for the LGBTQ+ community and has many restrictions. From our previous experience, we found working with such organizations challenging because of the complexity of the system and different regulations and compliances.
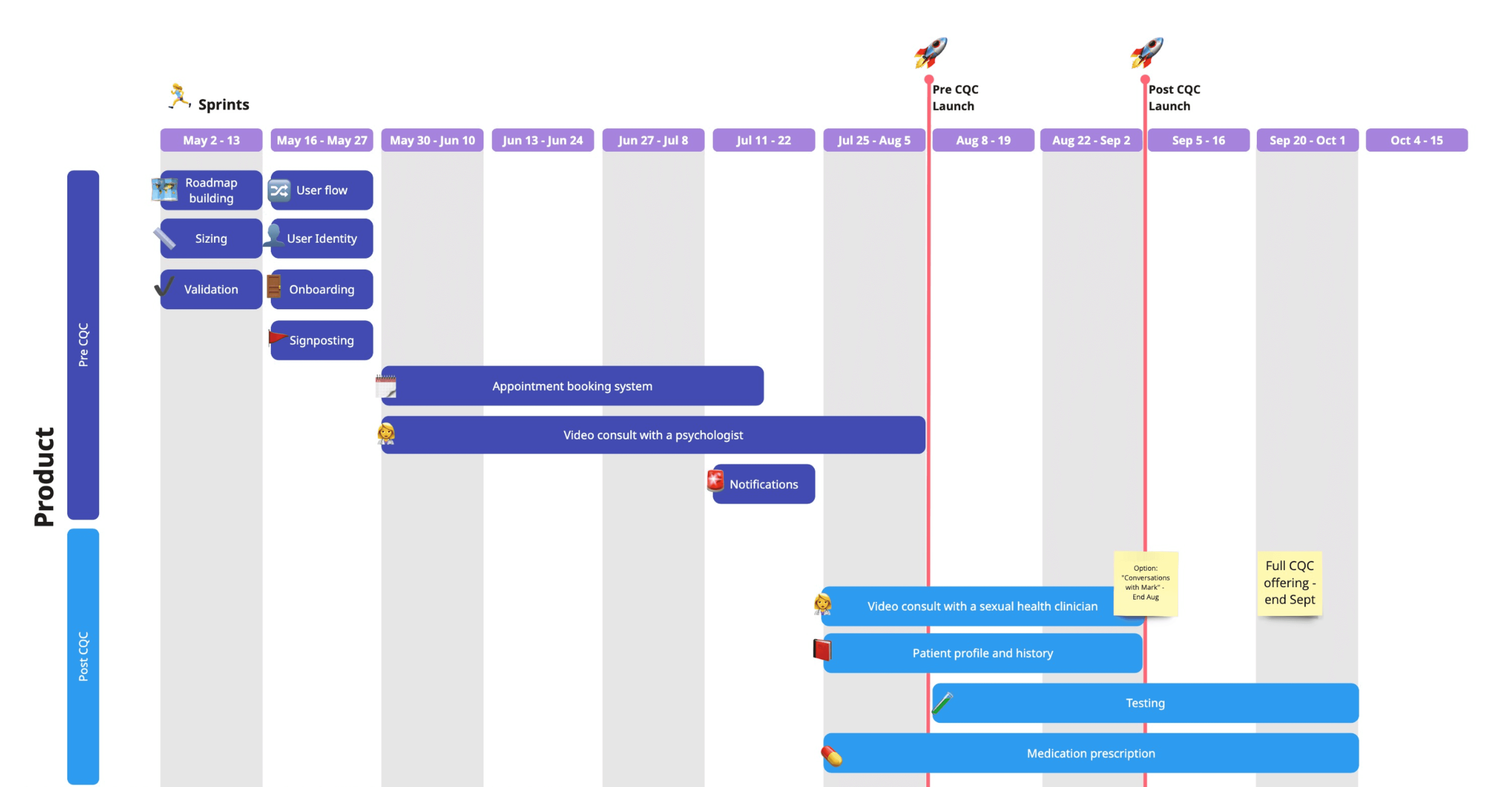
High-level roadmap
Next, we started defining different versions of the features we could build. This included the most straightforward version we could create with the least resources, high effort, full-fledged features, and others based on the effort required to make them. After prioritizing one of the features and their different versions, we started defining our high-level roadmap based on the importance of the features, the team’s capacity to build them, and other constraints, such as CQC registration and funds.
For phase 1, i.e., pre-COQ, we decided to work on the psychological and well-being features that do not require CQC registration. Phase 2 includes all the clinical services and the complementary features. We also had some features in the backlog that did not come under either of the phases and would be developed after the full-service launch. The reason to work on the features in these phases was to build something quickly and validate the product market fit.
Key goals
Provide LGBTQ+ affirming care without any stigma or discrimination, specifically tailored to the needs of the individuals.
Provide sexual health clinical services remotely efficiently and effectively.
Help LBGTQ+ people improve their mental wellbeing by providing tailored services and self-help resources.
Ensure the privacy and safety of the users.
Educate people about sexual health and mental wellbeing.
Defining the solution
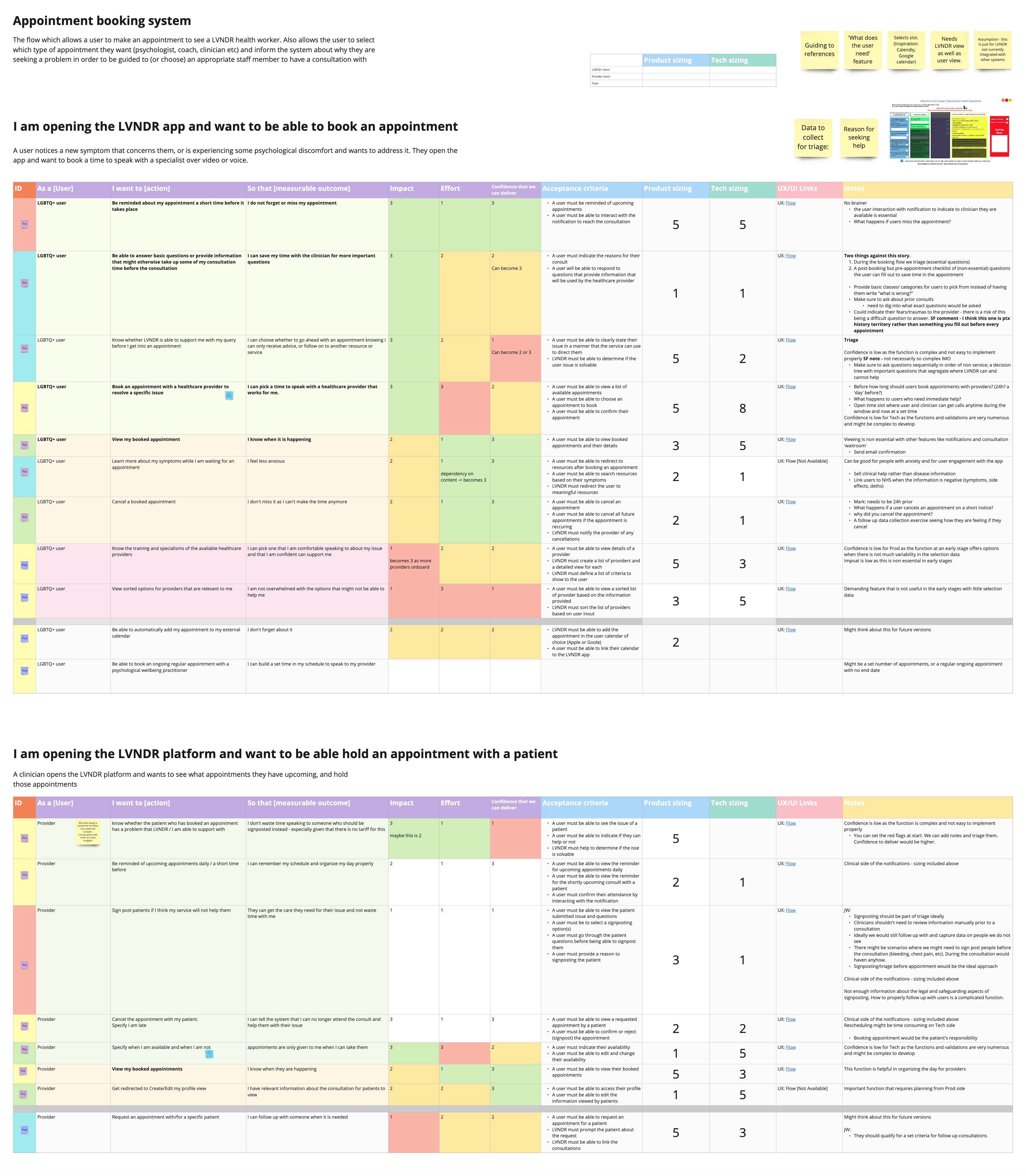
Defining features and user stories
Next, we started defining the features and user stories for them. Once we had all the user stories, we tagged them with pre-CQC and post-CQC tags, rating them on impact, effort, and confidence to deliver scales. We also defined and sized the acceptance criteria for product and engineering teams. We also defined user flows for each user story and discussed them with other LVNDR teams to get their feedback and insights into developing the features.

Feature sizing
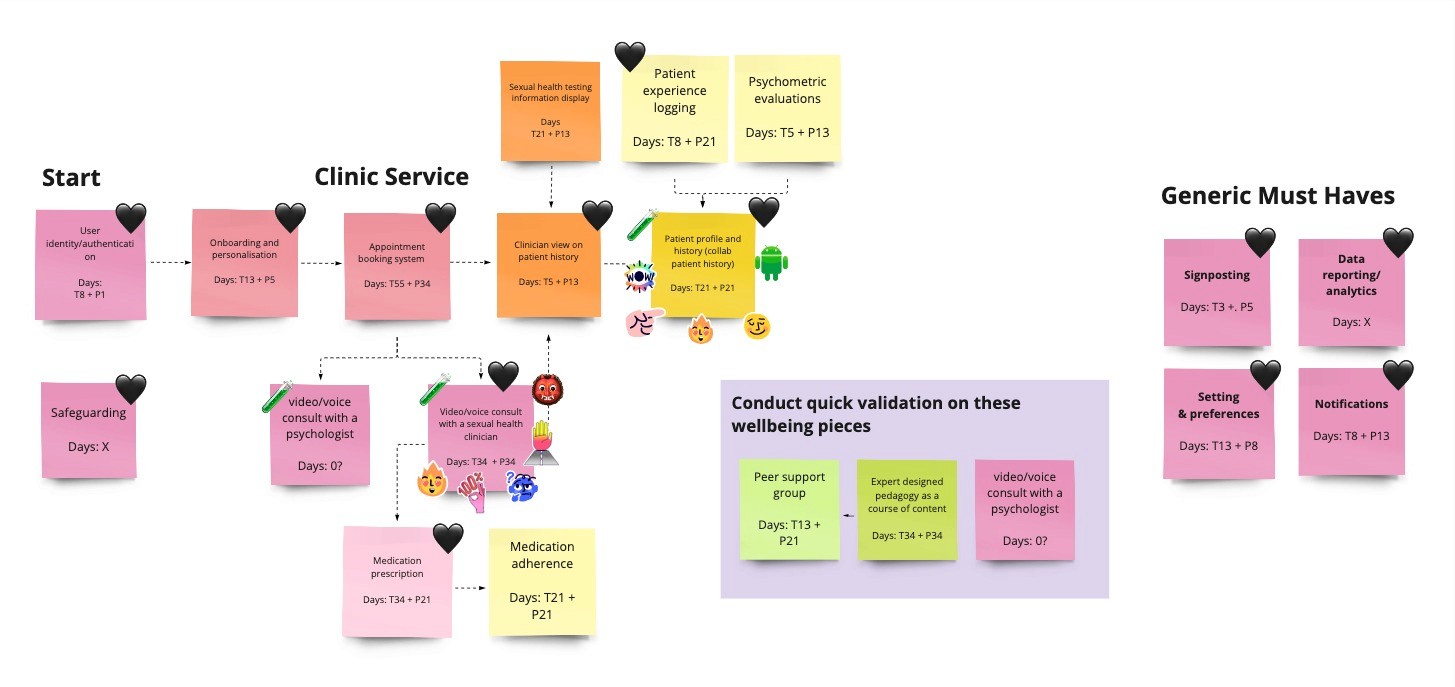
User flow/Sitemap
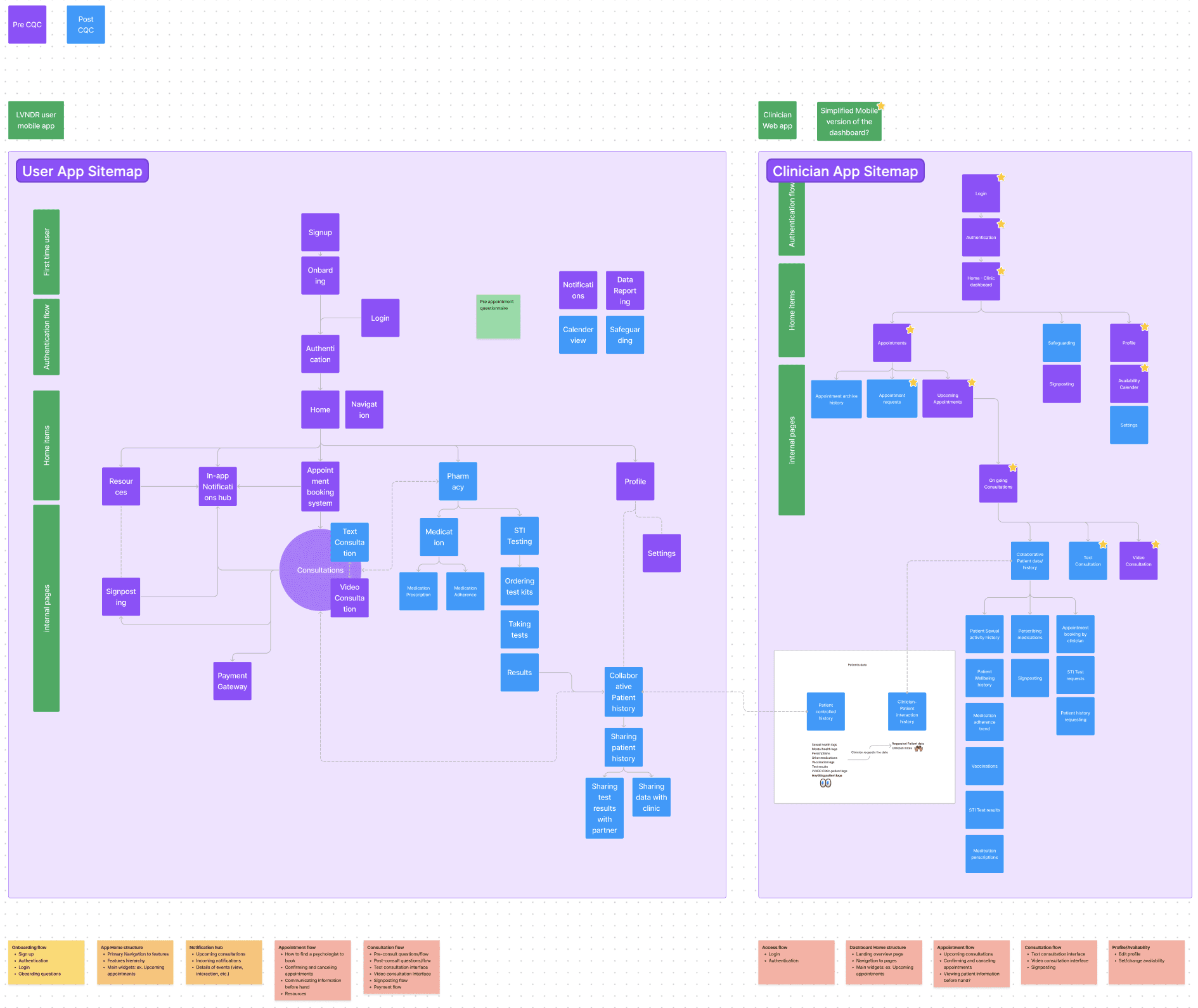
Prioritising roadmap
Prioritizing the features
Assigning the duties
Once we had a clear idea of the roadmap, we started breaking down the features into smaller sub-features and prioritizing them. We also created detailed user flows and sitemaps for the features. We conducted various sprints working on designing the features. At the start of each sprint, we prioritized the work and assigned duties among the Product team. This included collecting data and requirements, Collaborating with the clinical and engineering teams, producing the design deliverables, validating the designs, and maintaining an expansive and scalable design system.
Realignment
At a later stage, we had to rework the roadmap as we accelerated the CQC registration process. We decided to build the clinical consultation feature before the psychological consultation feature as this was a higher priority feature. These features overlapped a lot, so I did not have to start over again. We pushed back the psychological well-being features and started working on the clinical features. This required us to redefine our MVP into multiple phases. Phase 1 included appointments with clinicians for PrEP, initial STI screening, medication delivery, and payments. Phase 2 would focus on expanding the clinical offering, such as STI testing, STI treatments, other HIV medication, etc. Phase 3 would focus on providing psychological well-being features.













